

Background
Our knowledge of the outcome of patients with relapsed/refractory diffuse large B-cell lymphoma (R/R DLBCL) in the rituximab era is mostly derived from randomised controlled trials or specialized center cohorts presenting selected patient materials. With new targeted therapies being evaluated in the relapsed/refractory setting such as CART therapy, there is a need for a better understanding of the expected survival in real-world cohorts of R/R DLBCL and the likelihood of patients being selected for established intensive treatment schedules and consolidation with autologous stem cell transplantation (ASCT). Here we investigated timing of relapse, treatment intensity and outcome among patients with R/R DLBCL in a nationwide population-based cohort.
Methods
Patients with R/R DLBCL (N=713) were identified among all patients with a first incident DLBCL diagnosed 2007-2014 recorded in the Swedish Lymphoma Register and treated with primary anthracycline-based immunochemotherapy (N=3528), with follow-up until December 31st 2018. The register holds information about clinical characteristics at diagnosis, primary treatment, treatment response and relapse. Data regarding treatment response and relapse was validated through medical chart review in the entire cohort and information about second-line treatment and ASCT was collected. Timing of progression/relapse was categorized by time interval in months from diagnosis (0-12, 12-24, 24+). Treatment intensity was categorized in four groups: intensive chemotherapy (e.g., DHAP, ICE, GDP) with intent of ASCT, remission-inducing chemotherapy (e.g., GemOx, IME, Benda), palliative therapy (oral chemotherapy, radiotherapy) and no active antitumoral treatment (e.g., steroids, best supportive care). Second-line treatments could have been given with or without immunotherapy. Overall survival probabilities were estimated in the entire cohort and by age >/≤ 70 years using the Kaplan-Meier method.
Results
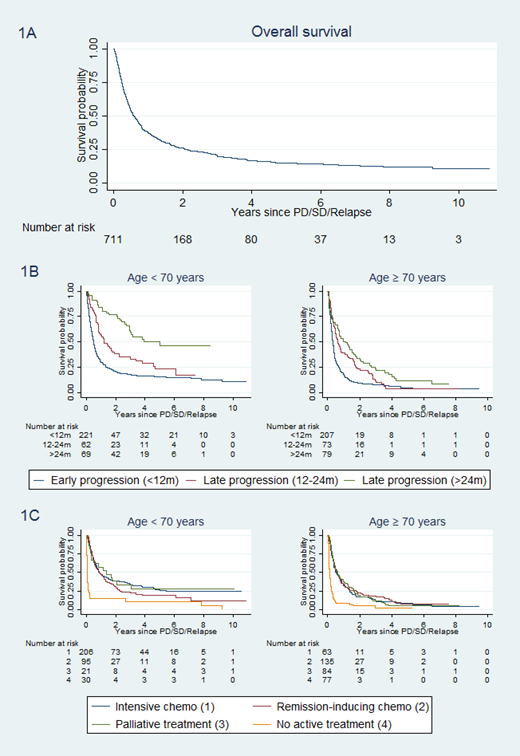
In the study population of 713 patients (59% men), median age at relapse was 71 years (range 18 to 95) and 61% had stage IV disease. Most patients relapsed within 12 months (N=428, 60%) whereas 135 patients (19%) relapsed 12-24 months from diagnosis and 148 patients (21%) after 24 months. In patients ≤70 years of age, intensive chemotherapy with intent of ASCT was started in 206 out of 354 patients (58%) and 124 (35%) subsequently received a consolidative ASCT. Remission-inducing chemotherapy was given to 95 patients (27%), 22 (6%) received palliative treatment directly and 31 (9%) were deemed unfit for any active treatment. Among patients >70 years at relapse, 63 patients started intensive chemotherapy (18%) and 4 (1%) were eventually transplanted, whereas another 127 (35%) received remission-inducing chemotherapy, 92 (26%) palliative therapy directly and 77 (21%) no active therapy. Overall survival in the entire cohort was 26% at 2 years (Figure 1A). Timing of relapse strongly correlated with survival, primarily among patients <70 years of age (2-year OS was 21% for 0-<12, 38% for 12-24 and 77% for 24+) (Figure 1B). By treatment intensity, outcomes also varied more among young patients in favor of the intensive chemotherapy with intent of ASCT (with 39% 2-year OS). Among young patients, timing of relapse correlated with the possibility to give consolidative ASCT (23% in early relapse vs >50% in relapse 12 months or after). Among patients >70 years, outcomes were strikingly poor in all treatment intensity groups (2-year OS 23% or lower).
Conclusion
In the population-based setting, less than 60% of patients with R/R DLBCL ≤70 years at relapse could go on to receive curative intent second-line treatment and only about one third were consolidated with ASCT (even fewer among those with early relapse). Among patients >70 years, outcomes were very poor and second-line treatment intensity seemed to have little impact on outcome, although there were a few longer-term survivors in all treatment groups. More efficient and less toxic therapies are urgently needed for R/R DLBCL at all ages.
Figure 1 A-C Overall survival of patients with relapsed/refractory diffuse large B-cell lymphoma in Sweden 2007-2014 (N=713) in the entire cohort (1A), by age >/≤ 70 years and timing of relapse (0-<12, 12-24, 24+ months of diagnosis) (1B) and by age >/≤ 70 years and treatment intensity categorized in 4 groups (1C).
Ekstroem Smedby:Janssen Cilag: Honoraria, Other: Grant funding, Research Funding; Celgene: Honoraria, Other: Grant funding, Research Funding; Takeda: Honoraria, Other: Grant funding, Research Funding. Ekberg:Swedish Cancer Society: Other: This project was partly funded by the Swedish Cancer Society; Janssen Pharmaceuticals: Other: This project was partly funded through a private-public collaboration between KI and Janssen pharmaceuticals.. Eloranta:Karolinska Institutet: Other: coordinator for a public-private real world evidence; Janssen Pharmaceuticals.: Other: project coordinator for a public-private real world evidence. Enblad:Kite/Gilead: Membership on an entity's Board of Directors or advisory committees. Jerkeman:Janssen: Honoraria, Research Funding; Gilead: Honoraria, Research Funding; Acerta: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; Roche: Honoraria, Research Funding. Andersson:Gilead: Research Funding; Gilead, Janssen and Roche: Consultancy; Abbvie and Janssen: Membership on an entity's Board of Directors or advisory committees. Harrysson:Swedish Cancer Society: Other: This project was partly funded by the Swedish Cancer Society.; Janssen pharmaceuticals: Other: This project was partly funded through a private-public collaboration between KI and Janssen pharmaceuticals..

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal