

Background: HIT has the potential to improve the health of individuals and the performance of providers, yielding improved quality, cost savings, and greater engagement by patients. Minorities face a variety of financial and nonfinancial barriers to obtaining appropriate and timely health care. Studying the behavior of minority patients will help understand the specific challenges to HIT adoption and engagement in patients and their caregivers. We undertook a patient-reported survey to explore these factors and understand any underlying disparities.
Methods: A 21-question paper-based anonymous questionnaire addressing the responder's attitudes, understanding and needs of the electronic medical record (EMR) was used. This was administered to adult patients with lymphoid malignancies and their caregivers at two campuses of Mayo Clinic in Florida (San Pablo and inner-city; Riverside). Categorical and continuous variables between white and minority responders as well as minority responders from the two campuses were compared using the Chi-square test and U Mann Whitney with a significance level of 0.05.
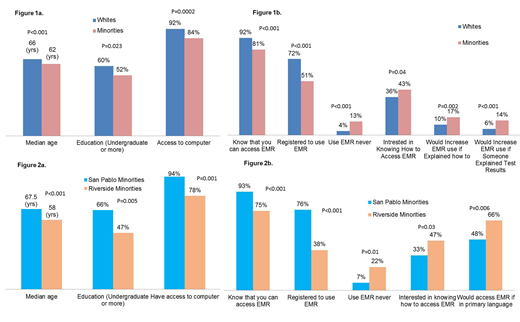
Results: The survey was completed by 1004 patients and caregivers. Average time taken to complete the survey was approximately 11 minutes. Of the responders, 716 (71%) were whites and 271 (27%) were minorities, with race-ethnicity not reported by 17 (2%). Among minorities, 30% (n=80) were seen at San Pablo and 64% (n=173) at the Riverside campus, with 6% at a multiple myeloma patient-caregiver symposium. Whites were older (median age 66 vs. 62 years, p<0.001) and had higher education (undergraduate or higher 60% vs. 52%, p=0.023) as compared to minorities. Minority survey responders had lesser access to a computer (84% vs. 92%, p<0.001) or a smartphone (85% vs. 89%, p=0.08). (Figure 1a) Exploring HIT awareness showed that only 51% of minorities were registered to use the EMR as compared to 72% whites (p<0.001) and a lesser number of minorities even knew that they could access their medical records electronically (81% vs. 92%, p<0.001). even among those registered to use the EMR, 13% minorities reported never using the EMR as compared to 4% whites (p<0.001). Encouragingly, a higher willingness to learn about and use the EMR was noted among minorities who were more interested in knowing how to access the EMR (43% vs. 36%, p=0.04), would increase the use of EMR if someone explained how to use it (17% vs. 10%, p=0.002), and if someone explained about test results (14% vs. 6%, p<0.001). (Figure 1b) Comparing minorities among the two campuses, those from the San Pablo campus were older (67.5 yrs. vs. 57 yrs., P<0.001), had higher level of education (undergraduate or higher in 66% vs. 47%, p=0.005) and a higher number had access to a computer (94% vs. 78%, P=0.001) as compared to those from the inner-city Riverside. (Figure 2a) Minorities from the Riverside campus were less likely to be aware of the current HIT EMR (75% vs. 93%, p<0.001), were significantly less likely to have registered for the patient EMR portal (38% vs. 76%, p<0.001) and never used the EMR even if registered for it (22% vs. 7%, p=0.01) as against those from the San Pablo campus. Minorities at the Riverside campus had a higher interest in knowing how to access the EMR (47% vs. 33%, p=0.03). Linguistic barriers were more striking in the inner-city Riverside campus where a higher proportion of minority survey responders noted that it would help if the EMR was in their primary language (66% vs. 48%, p=0.006). (Figure 2b)
Conclusions: Minorities continue to struggle with suboptimal utilization of healthcare system including that of HIT. There are barriers related to access, awareness, language and understanding of HIT that prevent the integration and participation of racial-ethnic minorities in the healthcare system to a full extent. It is important to qualify the minorities better, since there exist HIT utilization disparities even within the minorities from different areas representing socioeconomic and demographic differences. Efforts need to be made at several levels to help the minorities overcome educational, access and linguistic barriers so that they can benefit from advancements in the healthcare system.
Ailawadhi:Celgene: Consultancy; Amgen: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Pharmacyclics: Research Funding; Cellectar: Research Funding; Takeda: Consultancy. Manochakian:Novocure: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Membership on an entity's Board of Directors or advisory committees; Guardant Health: Membership on an entity's Board of Directors or advisory committees. Chanan-Khan:AbbVie: Research Funding; Xencor: Research Funding; Pharmacyclics: Research Funding; Merck: Research Funding; Jansen: Research Funding; Mayo Clinic: Employment; Ascentage: Research Funding; Millennium: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal