

Introduction: In the last decades, Hodgkin lymphoma (HL) has become a curable disease with a long-term disease-free survival achieved in about 80% of patients. The two main chemotherapy protocols presently used in HL treatment are: ABVD (adriamycin, bleomycin, vinblastine, dacarbazine) and escalated BEACOPP (EB) (bleomycin, etoposide, adriamycin, cyclophosphamide, vincristine, procarbazine, prednisone). Patients treated with ABVD also receive glucocorticoids to minimize regimen toxicity and as antiemetic prophylaxis. Similarly, prednisolone given for 14 days is an integral part of the EB regimen. However, glucocorticoids are known to interfere with bone formation and remodeling, which results in increased fracture risk. To reduce the rate of complications, such as aseptic necrosis of the femur head, according to the H2 Israeli protocol, patients treated with EB receive prednisone for seven days only. The current study was designed to evaluate the vertebral density (VD) changes associated with HL therapy.
Methods: In this retrospective study, data on all newly-diagnosed HL patients treated at the Rambam Health Care Campus between 2008-2016 were retrieved from the institutional computerized database. Patients were grouped based on their treatment protocol and further sub-grouped according to the number of treatment cycles: I ‒ ABVDx2-4, II ‒ ABVDx6, III ‒ EBx2+ABVDx4, IV ‒ EBx4-6+ABVDx2. VD findings of PET/CT scans performed at baseline and post-treatment were compared at L3 vertebral level. The Hounsfield unit (HU) scale was used to evaluate bone mineral density (BMD). The dose of hydrocortisone equivalents (HE) per meter square of the body surface area was calculated for each patient.
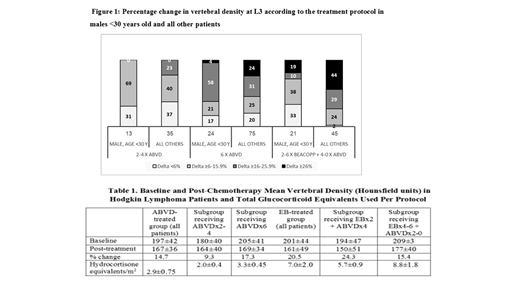
Results: All the identified newly-diagnosed HL patients (n=213) were included in the analysis. Their median age was 29 (18-59) years. Both baseline and post-treatment scan results were available for all patients. Mean VD at baseline was 198 HU (30.5-320) and post-treatment ‒ 165.5 HU (27.5-277.3). At baseline, 7 patients had osteopenia (<120 HU) and 1 patient had osteoporosis (<90 HU). The corresponding post-treatment numbers were 21 and 9 patients, respectively. Data on mean VD at baseline and post-therapy categorized according to the treatment received are presented in Table 1.
The mean VD change from the baseline level was 14.7% in the ABVD group as a whole, 9.3% HU in the ABVDx2-4 subgroup and 17.3% in the ABVDx6 subgroup. The mean VD change from the pre- to post-therapy level was 20.5% for the whole EB group, 24.3% for the EBx2 + ABVDx4 subgroup and 15.4% for the EBx4-6 + ABVDx2 subgroup.
The relative VD decreased post-treatment in all the subgroups. Using the ABVDx2-4 group as reference (HR=1), the HR for ABVDx6 group was 6.51 (95% CI 2.8-15.3; P=0.000), with HR=16.11 (95% CI 5.6-46.8; P=0.000) for EBx2 + ABVDx4 group and HR=2.78 (95% CI 0.9-8.2; P=0.065) for EBx4-6 + ABVDx2 group. There was a significant decrease in VD of 116 patients with HE >3.4gm/m2 compared to 24 patients with HE ≤2.1 gm/m2 (HR=6; 95% CI 2.1-17.2; P=0.001).
The present study demonstrated a bone density loss of ≥16% in 48% of patients and of ≥26% in 20% of patients. Osteopenia and osteoporosis developed in 7% and 4% of treated patients. Individuals receiving EBx6 had a less significant bone loss compared to those receiving EBx2 +ABVDx4. This could be explained in part by the older age (19% were above 46 years) of the latter patients. A similar VD loss of ≥16% was observed in patients treated with ABVDx6 and those receiving EB containing regimen (one week of steroids only) (56.6 and 59%, respectively).
A multivariate analysis for prediction of VD loss showed that age ≥30 (HR=2.19; 95% CI 1.13-4.24; P=0.02) and chemotherapy protocols other than ABVDx2-4 (ABVDx6: HR=6.65; 95% CI 2.80-15.78; P=0.000; BEACOPPx2-6: HR=7.87; 95% CI 3.14-19.71; P=0.000) were significant risk factors (Fig. 1).
Conclusions: The current study demonstrates that VD reduction is a significant problem in HL patients above the age of 30 years, treated with 6 cycles of chemotherapy containing HE >3.4gm/m2. As it may lead to osteopenia, a restrictive approach to the use of glucocorticoids should be applied in this patient population. These findings suggest that bone density should be followed in this group of HL survivors.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal