

Background - Combination of ibrutinib plus rituximab (IR) has generated significant efficacy and safety data in relapsed patients (pts) with MCL. In this single institution phase II trial, we investigated the efficacy and safety of using an IR combination followed by short course (4 cycles) of R-HCVAD/MTX-ara-C as consolidation in previously untreated young (age ≤ 65 years) pts with MCL. We hypothesized that using a chemo-free induction will mitigate the toxicities and risk of second cancers which are associated with the use of intensive chemoimmunotherapy regimen in these pts.
Methods - We enrolled 131 previously untreated young (≤65 years) pts with MCL. This study is registered with a ClinicalTrials.gov identifier number NCT02427620. Pts received IR induction (part-A), until they achieved complete remission (CR) for up to a maximum of 12 cycles, followed by a maximum of 4 cycles of R-HCVAD/R-MTX-ara-C (part-B) as consolidation. None of the patients received stem cell transplant or maintenance therapy. The primary objective was to assess overall response rate (ORR), [defined as either a partial response (PR) or a complete response (CR)] after part A. Adverse events were coded as per CTCAE version 4. Among evaluable samples, minimal residual disease (MRD) by flow cytometry at best response, clonal evolution using circulating tumor DNA (ctDNA), baseline somatic mutations and baseline gene expression profile (GEP) are being evaluated.
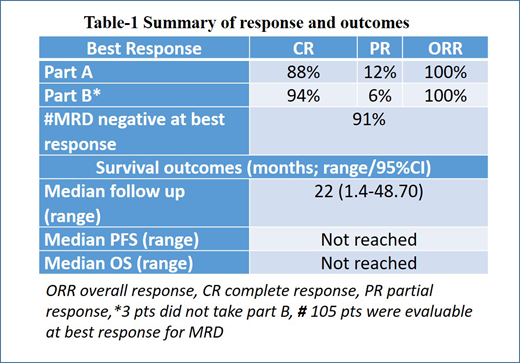
Results - Among the 131 pts, the median follow up was 22 months (1.4-48.70). Eighty percent were males. Median age was 56 yrs (range - 35-65). Forty nine percent had high Ki-67 (≥30%), 80% had low risk simplified MIPI score and 85% pts had initial marrow involvement. Fifteen pts had aggressive MCL (blastoid/pleomorphic), 17 pts had complex karyotype and 83% had positive SOX-11 expression. Median number of cycles on IR in part A was 7 (1-12). At week 16 on part A, the ORR was 95% (22% CR and 73% PR) and 5% pts had stable disease. Overall best response (ORR) on part A of therapy was 100% (88% CR and 12% PR) and at the time of last follow up after completion of part A and part B, ORR was 100% (94% CR). Among evaluable pts, MRD- negative CR rate assessed by bone marrow flow cytometry performed at best response at any phase of treatment was 78%. Among the 10 pts with TP53 mutations, 70% had a CR on part A alone. Overall, the median PFS and OS were not reached (3 year 85% and 97% respectively). Nine pts had relapsed after treatment, including 3 who transformed. Among these 9 pts, 7/9 pts had Ki-67% ≥ 30% and 3/9 pts had aggressive histology MCL. The PFS and OS were not significantly different among pts with high and low Ki-67% and among pts with/without achieving CR on part A and while PFS was significantly shorter in pts with aggressive MCL histology (p=0.005) but not the OS. Overall 3 pts died (one on study due to splenic hematoma, cardio-pulmonary arrest and was on IR for 1 month, one expired outside and was off study after discontinuation due to encephalitis and another expired outside and discontinued due to disease transformation). Twenty one pts came off study for various reasons [nine disease progression (including 3 transformation), 8 pt choice, 3 intolerance and one second cancer]. Grade 3-4 toxicities on part A were 4% myelosuppression and 8% each with fatigue, myalgia and rashes and 4% mucositis. None had grade 3-4 atrial fibrillation or bleeding. GEP was performed in 18 pts (2 PR, 16 CR on part A). Pts in PR had higher expression of HES1 while those in CR had significantly higher expression of CTLA4 and ITK genes compared with those in PR. Targeted DNA sequencing was done in 18 pts at baseline, one pt with PR had NSD2, KMT2C and another pt had TP53 mutations and had CR.
Conclusions - Excellent responses were observed with IR combination which is a chemo-free induction treatment strategy for young pts with MCL. This treatment approach has a strong potential to change the treatment paradigm in MCL pts to minimize the toxicity from chemoimmunotherapy without compromising the treatment efficacy and safety.
Wang:Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Pharmacyclics: Honoraria, Research Funding; Acerta Pharma: Consultancy, Research Funding; AstraZeneca: Consultancy, Honoraria, Research Funding, Speakers Bureau; VelosBio: Research Funding; Loxo Oncology: Research Funding; Celgene: Honoraria, Research Funding; Juno Therapeutics: Research Funding; Aviara: Research Funding; Dava Oncology: Honoraria; MoreHealth: Consultancy, Equity Ownership; BioInvent: Consultancy, Research Funding; Guidepoint Global: Consultancy; Kite Pharma: Consultancy, Research Funding. Lee:Seattle Genetics, Inc.: Research Funding. Westin:Genentech: Other: Advisory Board, Research Funding; Curis: Other: Advisory Board, Research Funding; Unum: Research Funding; 47 Inc: Research Funding; Janssen: Other: Advisory Board, Research Funding; Novartis: Other: Advisory Board, Research Funding; Juno: Other: Advisory Board; Celgene: Other: Advisory Board, Research Funding; MorphoSys: Other: Advisory Board; Kite: Other: Advisory Board, Research Funding. Nastoupil:Bayer: Honoraria; Celgene: Honoraria, Research Funding; Gilead: Honoraria; Genentech, Inc.: Honoraria, Research Funding; Novartis: Honoraria; TG Therapeutics: Honoraria, Research Funding; Spectrum: Honoraria; Janssen: Honoraria, Research Funding. Neelapu:Precision Biosciences: Consultancy; Kite, a Gilead Company: Consultancy, Research Funding; Merck: Consultancy, Research Funding; Unum Therapeutics: Consultancy, Research Funding; Poseida: Research Funding; Cell Medica: Consultancy; Karus: Research Funding; Acerta: Research Funding; Pfizer: Consultancy; Celgene: Consultancy, Research Funding; Novartis: Consultancy; Cellectis: Research Funding; Incyte: Consultancy; Allogene: Consultancy; BMS: Research Funding. Fowler:TG Therapeutics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Abbvie: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal