

Background: Treatment of Ph+ ALL has significantly improved since the addition of TKIs to chemotherapy, with improvement in complete molecular remission (CMR) and overall survival (OS) rates. However, the optimal duration of TKI is not yet established and the common practice is to continue indefinitely unless allogeneic stem cell transplant (ASCT) is performed. In pediatric setting, when TKIs were discontinued after 2 years of maintenance, high rates of relapse were seen, fortunately salvaged with ASCT and other approaches (Slayton WB et al; JCO. 2018 and Schultz KR; Leukemia 2014). In chronic myeloid leukemia, patients (pts) who achieve deep and sustained molecular remissions on TKI may be able to stop therapy successfully. Herein, we reviewed outcome of pts with Ph+ ALL treated with chemotherapy + TKI without ASCT who later discontinued TKI mainly due to adverse events.
Methods: We reviewed 240 pts treated at our institution on sequential protocols with Hyper-CVAD chemotherapy + TKI (dasatinib [n=100], ponatinib [n=84], or imatinib [n=56]) between 2001 and 2019. We identified 9 pts (4%) in whom TKI was discontinued, 4 (44.5%) post dasatinib therapy, 4 (44.5%) post imatinib therapy, and 1 (11%) post ponatinib. We analyzed their characteristics and outcomes including molecular relapse rates and treatment-free remission (TFR). Pts were closely monitored with monthly PCR for the first 3 months, then every other month for 3 months, then every 3 months thereafter. Molecular relapse was defined as the loss of MMR (PCR>0.1%) or positivity of PCR at two assessments within a 2-week period. TKI was resumed upon molecular relapse. TFR was defined from the date of TKI discontinuation to molecular relapse or last-follow-up. Kaplan-Meier method was used for survival analysis.
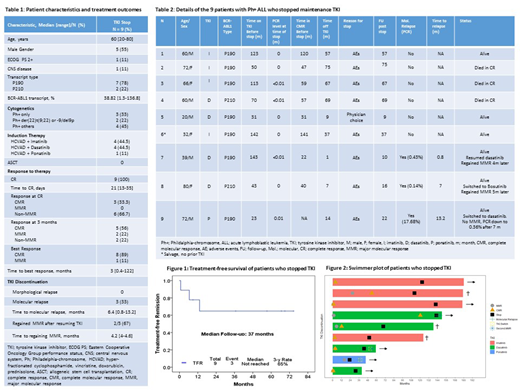
Results: Baseline characteristics are summarized in table 1. The median follow up from the time of diagnosis was 138 months (range: 40-190). The median age at diagnosis was 60 years (range: 20-80). Transcript type was p190 BCR-ABL1 in 7 pts (78%). Median time to CMR was 3 months (range: 0.4-120). Median duration of TKI therapy prior to discontinuation was 70 months (range: 23-143). Median duration of CMR before TKI stop was 52 months (range: 22-141). Reasons for stopping TKI were side effects in 8/9 pts, and physician's choice in 1 pt (after completing 2+ years of maintenance). At the time of TKI stop, 8 pts were in CMR, and 1 pt with low positive transcript level (0.01%). Median follow-up post TKI discontinuation was 37 months (range: 9-75). None of the pts had morphological relapse. Three pts (33%) had molecular relapse within a median of 6 months (range: 0.8-13.2 months). All 3 resumed TKI therapy: 2 of them regained MMR after a median of 4 months (range: 4.0-4.6 months); third pt continues to respond; the BCR-ABL1 transcripts down from 17.68% to 0.36% after 7 months (Table 2). Six pts remain alive and 3 pts died of disease-unrelated causes. The median TFR was not reached; 3-y TFR was 65% (Figure 1). Though the number of pts was only 9, the duration of CMR had a tendency of successful TFR (P=0.062; HR, 0.09; [95% CI, 0.009-1.119] with duration of CMR for 2 years, and P=0.137; HR, 0.15; [95% CI, 0.01-1.80] with duration of CMR for 3 years, as a binomial variable). The median duration of CMR in pts who relapsed and who did not relapse was 22 months (range, 0-39.9) and 58 months (range, 30.9-140.6), respectively (P= 0.096).
Conclusions: Our anecdotal experience reflects the feasibility of stopping TKI in a subset of pts with Ph+ ALL and sustained molecular remissions. Longer follow up and validation of these findings on a larger cohort are highly needed before attempting to discontinue TKI.
Kantarjian:Astex: Research Funding; Ariad: Research Funding; Jazz Pharma: Research Funding; AbbVie: Honoraria, Research Funding; Cyclacel: Research Funding; Immunogen: Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; BMS: Research Funding; Takeda: Honoraria; Agios: Honoraria, Research Funding; Novartis: Research Funding; Amgen: Honoraria, Research Funding; Pfizer: Honoraria, Research Funding; Daiichi-Sankyo: Research Funding. Sasaki:Otsuka: Honoraria; Pfizer: Consultancy. Konopleva:Ascentage: Research Funding; Reata Pharmaceuticals: Equity Ownership, Patents & Royalties; Agios: Research Funding; Ablynx: Research Funding; Cellectis: Research Funding; Amgen: Consultancy, Honoraria; F. Hoffman La-Roche: Consultancy, Honoraria, Research Funding; Calithera: Research Funding; Stemline Therapeutics: Consultancy, Honoraria, Research Funding; Forty-Seven: Consultancy, Honoraria; Eli Lilly: Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Kisoji: Consultancy, Honoraria; Astra Zeneca: Research Funding; Genentech: Honoraria, Research Funding. O'Brien:Acerta: Research Funding; AbbVie: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria, Research Funding; Sunesis: Consultancy, Research Funding; Janssen: Consultancy, Honoraria; Kite: Research Funding; GlaxoSmithKline: Consultancy; Gilead: Consultancy, Research Funding; Eisai: Consultancy; Celgene: Consultancy; Astellas: Consultancy; Aptose Biosciences, Inc: Consultancy; Amgen: Consultancy; Alexion: Consultancy; TG Therapeutics: Consultancy, Research Funding; Vaniam Group LLC: Consultancy; Verastem: Consultancy; Regeneron: Research Funding; Pharmacyclics LLC, an AbbVie Company: Consultancy, Research Funding. Kadia:Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding; Jazz: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Research Funding; Bioline RX: Research Funding; BMS: Research Funding; Amgen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Genentech: Membership on an entity's Board of Directors or advisory committees; Pharmacyclics: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; AbbVie: Consultancy, Research Funding. Jabbour:Takeda: Consultancy, Research Funding; BMS: Consultancy, Research Funding; Adaptive: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Cyclacel LTD: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal