

Introduction
Limited stage disease accounts for 30-40% of Diffuse Large B-cell Lymphoma (DLBCL), with better overall survival than advanced stage disease, but with increased late relapses regardless of treatment strategy (Stephens 2016). Preferred treatment for these patients (pts) per NCCN guidelines is abbreviated R-CHOP followed by radiotherapy. Based on promising results of radioimmunotherapy consolidation in SWOG S0313 (Persky 2015), and of PET-directed experience by the BC Cancer Agency (Sehn 2011), we designed a National Clinical Trials Network (NCTN) PET-directed study to tailor therapy after 3 cycles of R-CHOP, to improve outcomes and decrease toxicities.
Methods
Pts had non-bulky (< 10 cm) stage I/II untreated DLBCL. Mediastinal, HIV-associated, testicular, central nervous system, and indolent lymphoma were excluded. Pts received standard R-CHOP therapy and had an interim PET scan on day 15-18 of cycle 3, which was centrally reviewed in real time. Pts with negative PET scan (Deauville 1-3, iPET-neg) proceeded with 1 additional cycle of R-CHOP. Pts with positive PET scan (Deauville 4-5, iPET-pos) initiated 36 Gy of involved field radiation therapy (IFRT), plus additional boost to FDG-avid area up to 9 Gy, within 5 weeks of 3rd cycle of R-CHOP. This was followed by ibritumomab tiuxetan (IFRT-Zevalin) 3-6 weeks after completing IFRT. Final PET scan was performed 12 weeks after treatment completion.
Results
The study completed accrual in June 2016. Safety, response, interim PET, and immunohistochemistry-based cell of origin (COO) and MYC/BCL2 analyses were presented previously (Persky 2017, Stephens 2017).
Of 159 pts enrolled, 1 was upstaged by PET, and 26 pts were ineligible - due to incorrect histology (mostly concurrent indolent or follicular lymphoma grade 3B) (21), lack of diagnostic tissue submission for central pathology review (3), and bulky disease (2).
In 132 eligible pts, median age was 62 years, 62% had stage I, 17% had B symptoms, 14% had elevated LDH, 43% had extranodal involvement, and 66% had exclusive involvement of the head and neck region. Stage modified IPI (smIPI, Miller 1998) was 0 in 27%, 1 in 42%, 2 in 28%, and 3 in 4% of the pts. COO by Lymph2Cx was assessable in 87 pts - 68% were GCB, 23% were ABC, and 9% were unclassifiable. Double protein expressers (MYC and BCL2, DPE) were 16%, while 4 (3%) pts had "double hit" lymphoma (DHL) - 2 with MYC/BCL2 and 2 with MYC/BCL6 rearrangements - none of which were DPE.
Of 132 eligible pts, 128 had an interim PET scan centrally reviewed, of which 110 were iPET-neg. Only 18 were iPET-pos, 4 of them due to infection (Deauville X) which were treated as iPET-neg. Of 14 truly iPET-pos pts (11%), 2 refused radiation, and 12 pts received IFRT-Zevalin. Eight pts (67%) converted from PR to CR after IFRT-Zevalin and 4 (33%) had PR, for an overall CR of 92% and PR of 4% (with 4% unevaluable).
With median follow up of 4.5 yrs (range 1.1 - 7.5 yrs), only 5 pts progressed and 2 died from lymphoma. Of 5 progressors, 3 received R-CHOP x 4, 1 was iPET-pos but declined radiation, and 1 went off treatment after 1 cycle of R-CHOP. Eleven pts died from non-lymphoma causes, including 1 pt from secondary AML (iPET-neg arm), and 1 of lung adenocarcinoma diagnosed upon iPET.
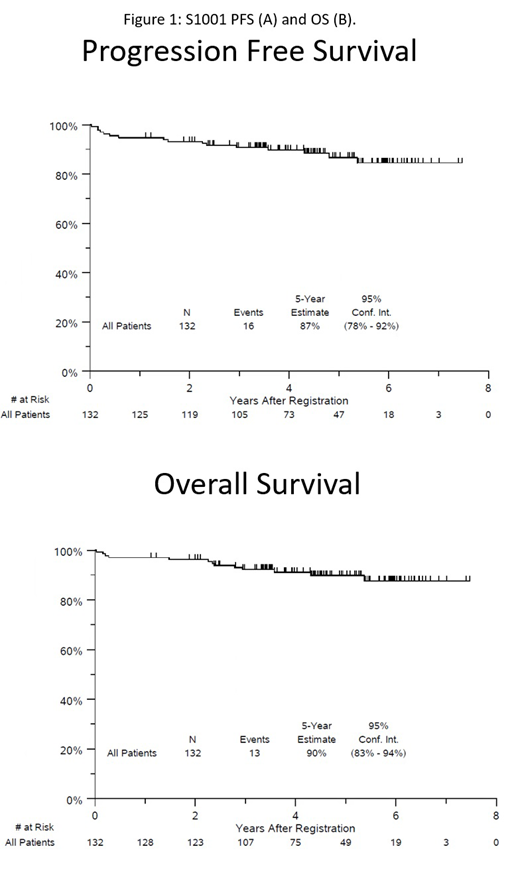
S1001 5-yr PFS estimate is 87% and OS estimate is 90% (figure 1), with iPET-pos and iPET-neg pts having similar outcomes - PFS 86% vs. 88%, OS 93% vs. 91%, respectively. Five-yr PFS by smIPI was 97% for smIPI of 0, 86% for 1-2, and 30% for 3. GCB had 5-yr PFS of 95%, vs. 70% for ABC and 47% for unclassifiable. DPE pts had 5-yr PFS of 70, vs. 89% for non-DPE pts. All 4 DHL pts maintain remission.
Conclusions
S1001 is the largest US study of limited stage DLBCL in the rituximab era, with best NCTN results in this disease subset. Only 5 patients progressed and 2 died from lymphoma. Our study confirms the distinct biology of limited stage DLBCL, with predominance of GCB origin (68%), and head and neck location (66%). Due to small number of lymphoma events, no strong conclusions about prognostic ability of smIPI, COO, DPE, or DHL, could be made.
S1001 demonstrated that 89% of pts maintained excellent outcomes after R-CHOP x 4 with PET-directed therapy. Only 11% of pts were iPET-pos and required radiation, but they also had excellent outcomes. Together with the FLYER trial in younger pts (Poeschel 2018), this NCTN trial establishes R-CHOP x 4 alone as the new standard approach to limited stage disease for majority of the pts.
Persky:Sandoz: Consultancy; Morphosys: Other: Member, Independent Data Monitoring Committee; Debiopharm: Other: Member, Independent Data Monitoring Committee; Bayer: Consultancy. Stephens:Acerta: Research Funding; Karyopharm: Research Funding; Gilead: Research Funding. Park:BMS: Consultancy, Research Funding; Rafael Pharma: Membership on an entity's Board of Directors or advisory committees; G1 Therapeutics: Consultancy; Teva: Consultancy, Research Funding; Gilead: Speakers Bureau; Seattle Genetics: Research Funding, Speakers Bureau. Bartlett:Seattle Genetics: Research Funding; ADC Therapeutics: Consultancy, Research Funding; Pfizer: Research Funding; Millenium: Research Funding; Bristol-Myers Squibb: Research Funding; Celgene: Research Funding; Genenetech: Research Funding; Immune Design: Research Funding; Gilead: Research Funding; Forty Seven: Research Funding; Janssen: Research Funding; Affimed: Research Funding; Merck: Research Funding; Pharmacyclics: Research Funding. Swinnen:Pharmacyclics: Consultancy; AbbVie: Consultancy. Barr:Celgene: Consultancy; Merck: Consultancy; Seattle Genetics: Consultancy; Genentech: Consultancy; Verastem: Consultancy; Gilead: Consultancy; Astra Zeneca: Consultancy, Research Funding; Janssen: Consultancy; AbbVie: Consultancy; Pharmacyclics LLC, an AbbVie company: Consultancy, Research Funding; TG Therapeutics: Consultancy, Research Funding. Leonard:Nordic Nanovector: Consultancy; Akcea Therapeutics: Consultancy; BeiGene: Consultancy; Gilead: Consultancy; Miltenyi: Consultancy; ADC Therapeutics: Consultancy; Nordic Nanovector: Consultancy; Akcea Therapeutics: Consultancy; Sandoz: Consultancy; ADC Therapeutics: Consultancy; Miltenyi: Consultancy; Genentech, Inc./F. Hoffmann-La Roche Ltd: Consultancy; Karyopharm Therapeutics: Consultancy; Epizyme, Inc: Consultancy; Sutro Biopharma: Consultancy; AstraZeneca: Consultancy; AstraZeneca: Consultancy; Bayer Corporation: Consultancy; Bayer Corporation: Consultancy; Celgene: Consultancy; Epizyme, Inc: Consultancy; Celgene: Consultancy; Genentech, Inc./F. Hoffmann-La Roche Ltd: Consultancy; Merck: Consultancy; MorphoSys: Consultancy; Karyopharm Therapeutics: Consultancy; Gilead: Consultancy; Sutro Biopharma: Consultancy; BeiGene: Consultancy; Merck: Consultancy; MorphoSys: Consultancy; Sandoz: Consultancy. Kahl:TG Therapeutics: Consultancy; ADC Therapeutics: Consultancy, Research Funding; Seattle Genetics: Consultancy; BeiGene: Consultancy. Fisher:Celgene: Consultancy; AstraZeneca: Consultancy; Barclays: Honoraria; prIME: Honoraria. Rimsza:NanoSting: Patents & Royalties: Named inventor on a patent licensed to NanoSting [Institution]. Smith:Portola Pharmaceuticals: Research Funding. Friedberg:Bayer: Honoraria, Other: Data & Safety Monitoring Committee; Acerta: Other: Data & Safety Monitoring Committee.
Ibritumomab tiuxetan in diffuse large B-cell lymphoma

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal