

Introduction: Primary hemophagocytic lymphohistiocytosis (HLH) has historically been associated with a number of genetic mutations resulting in impaired lymphocyte cytotoxicity. More recently, we have learned that defects of the inflammasome immune complex, such as in X-linked inhibitor of apoptosis (XIAP) deficiency, cause an HLH phenotype with normal cytotoxic function and that patients with XIAP deficiency have a high risk of peri-transplant HLH flare and mortality. This study aims to further elucidate the differential peri-transplant courses of HLH patients depending on their underlying genetic backgrounds.
Methods: We retrospectively extracted data from medical records of patients who underwent allogeneic hematopoietic cell transplant (HCT) for HLH or an HLH-predisposing immunodeficiency at UCSF Benioff Children's Hospital between 2006-2018. Event-free survival (EFS) was defined as successful engraftment without rejection or failure of initial transplant. HLH recurrence was defined by HLH-2004 diagnostic criteria. All time ranges were measured from the date of HCT admission. Log rank tests were used for statistical testing of survival data.
Results: We identified 23 subjects, median age 4 years (0.4-22.5 years). 13/23 (57%) were found to have a pathogenic variant in a non-inflammasome, HLH-associated gene ("Proven Typical HLH"), 2/23 (9%) had mutations involving the inflammasome ("Proven Atypical HLH," both with XIAP deficiency), and 8/23 (35%) had no identified genetic defect ("Possible Atypical HLH"). The latter two groups were analyzed as "Atypical HLH." The majority of patients received conditioning with busulfan, fludarabine, and alemtuzumab.
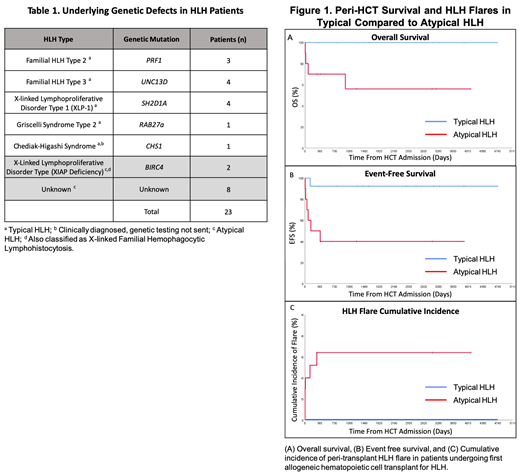
With median follow up of 4.3 years, 3-year overall survival was 82% (95% CI, 65-98%). The 3-year EFS was 69% (95% CI, 50-88%). In engrafted patients (21/23, 91%), median donor myeloid chimerism (30-day, 100%; 180-day, 100%; 365-day 99%) and T cell chimerism (30-day, 76%; 180-day, 97%, 365-day 99%) were high. The cumulative incidence of grade II-IV acute GvHD in transplant recipients was 15% (95% CI, 0-30%). 3-year OS and EFS were both significantly higher in Typical HLH patients at 100% (95% CI, 75-100%) and 92% (95% CI, 78-100%), respectively, compared to Atypical HLH patients whose OS and EFS were 56% (95% CI, 23-90%) and 40% (95% CI, 10-70%), respectively (p=0.006 and 0.011). The only event in the Typical HLH group was a primary graft rejection, salvaged with second HCT. Peri-transplant mortality occurred only in patients without a known mutation (53%; 95% CI, 16-90%) compared to those with known mutations (0%; 95% CI, 0-25%; p=0.002). 3-year HLH-free survival was also significantly (p<0.001) higher in Typical HLH patients (100%; 95% CI, 75-100%) compared to Atypical HLH patients (30%; 95% CI, 2-58%), as peri-transplant HLH flares occurred only in the Atypical HLH group, with half (3/6) surviving the flare. All flares occurred within 1 year of HCT admission (range 2-291 days), and all events occurred within 3 years of admission (range 5-993 days).
Conclusions: HLH is a clinical phenotype with significant underlying genetic heterogeneity, manifested in differential peri-transplant outcomes. Patients with proven Typical HLH have improved survival and EFS as well as decreased risk of peri-transplant HLH compared to those with proven or possible Atypical HLH. Given limitations in current testing, it is possible that patients without a known defect in the cytotoxic pathway may have underlying inflammasome mutations. Defects in XIAP and the resulting loss of apoptosis protection appear to put patients at higher risk of chemotherapy complications. These results demonstrate the need for thorough genetic testing in all HLH patients prior to HCT, as well as close monitoring for development of a peri-HCT flare in patients without proven Typical HLH. If validated in a larger dataset, patients with proven or possible Atypical HLH may be considered for trials of anti-cytokine therapy in the peri-transplant period.
Shimano:Pfizer: Research Funding; Novartis: Research Funding; Daiichi Sankyo: Research Funding. Huang:Novartis: Research Funding. Dvorak:Alexion Inc: Consultancy; Jazz Pharmaceuticals: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal