

INTRODUCTION: Allogeneic blood or marrow transplant (alloBMT) is widely used in relapsed/refractory systemic non-Hodgkin lymphoma. The graft-versus-tumor effect has been thought to be blunted by the immune privilege of the central nervous system (CNS). Communication between the CNS and the systemic immune system suggests that CNS disease could benefit from the graft versus lymphoma (GVL) effect provided by alloBMT.
METHODS: The charts of all patients who received post-transplant cyclophosphamide (PTCy)-based graft-versus-host disease (GVHD) prophylaxis between January 2004 and October 2018 were reviewed. Survival statistics were calculated using the Kaplan-Meier method. Differences in time to death between groups were estimated using Cox proportional hazards models.
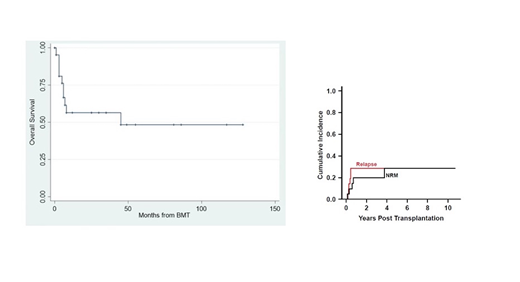
RESULTS: Twenty-one patients with systemic lymphoma involving the CNS were identified. The median age was 59 years (range 24-73); 7 were over the age of 60 and 13 were male. Histology types included diffuse large B cell (71%), Burkitt (10%), T cell (10%), follicular (5%), and anaplastic large cell (5%). Prior to transplant, 12 patients were in complete remission, 9 had residual disease, and 5 had residual CNS disease by imaging. Induction therapy included CNS radiation therapy in 11 of 21 patients (52%) and high-dose methotrexate (HD-MTX) in 10 (48%). Only 1 patient was in first remission, with the remaining 20 in second or later remission. All but 1 patient received non-myeloablative conditioning using fludarabine, cyclophosphamide, and total-body irradiation; the other patient received busulfan and cyclophosphamide. Fifteen patients (71%) had haploidentical donors. Graft source was bone marrow in 18 patients and G-CSF-stimulated peripheral blood in 3. Median overall survival (OS) for the entire cohort was 1375 days (95% confidence interval [CI] 184-NR) and median progression free survival (PFS) was 1375 days (95% CI 112-NR). Three-year overall survival was 51% (95% CI 27-71%). The cumulative incidence of relapse was 29% (95% CI 9-49%) at 3 years, and non-relapse mortality was 20% (95% CI 2-38%) at 1 year. Of the 6 patients who relapsed, 2 were CNS only, 2 were systemic only, and 2 were combined CNS / systemic. There were 2 cases of grade III-IV acute GVHD and 1 case of chronic GVHD involving the mouth. Univariable analysis revealed no predictors of survival in our small data set: age > 60 (hazard ratio [HR] 1.48, 95% CI 0.42-5.29, p-value 0.54), haploidentical donor (HR 4.2, 95% CI 0.53-33.66, p-value 0.17), residual disease (HR 1.3, CI 0.37-4.52, p-value 0.68), and prior CNS radiation (HR 1.5, 95% CI 0.42-5.31, p-value 0.53).
DISCUSSION: Allogeneic BMT with non-myeloablative conditioning is potentially curative in patients with secondary CNS lymphoma. Post-transplant cyclophosphamide is well tolerated in this older group. Myeloablative conditioning directed at the CNS is not required for long-term survival. Given its biologic plausibility and potential as a viable treatment option in certain patient populations, the role of alloBMT in CNS lymphoma deserves further investigation.
Wagner-Johnston:ADC Therapeutics: Membership on an entity's Board of Directors or advisory committees; Jannsen: Membership on an entity's Board of Directors or advisory committees; Gilead: Membership on an entity's Board of Directors or advisory committees; Bayer: Membership on an entity's Board of Directors or advisory committees. Swinnen:Pharmacyclics: Consultancy; AbbVie: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal