


Background
The intensity of a conditioning regimen has significant impact on outcomes of allogeneic hematopoietic cell transplantation in acute leukemia. In acute lymphoblastic leukemia (ALL) patients undergoing matched donor transplant, total body irradiation (TBI)- based myeloablative conditioning (MAC) regimen was associated with improved leukemia free survival (LFS) compared to chemotherapy (CT)-based MAC (Eder S. et al. 2017). Haploidentical hematopoietic cell transplantation(haplo-HCT) with post-transplant cyclophosphamide (PTCy) has emerged as a safe alternative in absence of a matched donor. The optimal MAC in haplo-HCT setting is yet to be defined. We studied the outcomes of TBI- vs. CT-based MAC in ALL patients undergoing haplo-HCT and reported to the Acute Leukemia Working Party of the EBMT.
Methods
The study included 427 ALL (B-ALL-75%) patients, that underwent haplo-HCT with PTCy during the years 2010-2018, following TBI- (n=188, 44%) or CT- (n=239, 56%) based MAC. Regimen intensity was defined by EBMT criteria and cases with busulfan dose <9 mg/kg or TBI dose ≤6 Gy were excluded. All disease status were included (CR1=208, CR2+=135; advanced=84). Ninety-one (27%) patients had Philadelphia+ disease. Graft source was bone marrow in 229 (54%) patients. Fludarabine-TBI (72%) and thiotepa-busulfan-fludarabine (65%) were the most common TBI and CT-based regimens, respectively. Cyclosporin with mycophenolate was used as GVHD prophylaxis in 64% of patients. The patients, disease, and transplant related characteristics were similar in both cohorts. Median patient age was 32 yrs and the median follow ups for TBI and CT cohort were 20.7 (IQR-11.7-35.3) and 26.2 (IQR-10.2-41) months, respectively.
Results
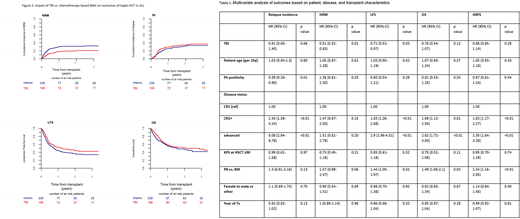
In univariate analysis, day 100 incidences of acute GVHD II-IV and III-VI were 38% vs. 30% (p-0.07) and 19% vs. 13% (p-0.14) for TBI and CT cohort, respectively. Two-year overall and severe chronic GVHD incidences were 34% vs. 30% (p-0.51) and 17% vs. 12% (p-0.18) for TBI and CT cohort, respectively. Graft failure was reported in 6 (3%) and 19 (8%)(p-0.09) patients who received TBI and CT-based MAC, respectively. Death from veno-occlusive disease was reported in 4 (5%) TBI patients and 8 (7%) CT patients. There was no difference in reported deaths due to infection (28%) or interstitial pneumonitis (4%) among study cohorts. In multivariate analysis, TBI was associated with significant improvement in nonrelapse mortality (NRM) [HR=0.51, 95% CI:0.32-0.83, p<0.01] and LFS [HR=0.71, 95% CI:0.52-0.97, p-0.03] and higher incidence of aGVHD II-IV [HR=1.5, 95% CI:1.02-2.19, p-0.04]. Finally, relapse incidence (RI), acute GVHD (aGVHD) III-IV, OS and GVHD free relapse free survival (GRFS) did not differ between the groups. Two-year NRM, LFS and OS of TBI and CT cohort were 21% vs. 31% (p<0.01); 45% vs. 37% (p-0.05) and 51% vs. 47% (p-0.18), respectively (Figure 1). Other factors negatively impacting OS were disease status (CR2, HR=1.69, p-0.01 or advance, HR=2.62, p<0.01) and use of peripheral blood as graft source (HR=1.49, p-0.02). Interestingly, peripheral blood graft source also negatively impacted LFS (HR=1.44, p-0.02), aGVHD II-IV (HR=1.58, p-0.02 and GRFS (HR=1.54, p<0.01). Philadelphia+ disease was associated with reduced RI (HR=0.39, p-0.01) but had no impact on LFS (HR=0.80, p-0.29) or OS (HR=0.81, p-0.34)(Table 1).
In a subgroup univariate analysis of patients <40 yrs old, TBI was associated with reduced 2-year NRM (19% vs. 28%, p-0.04) without impacting other outcome measures. In patients with pre-HCT disease status CR2 or advance disease, improvement in 2-year NRM (22% vs. 36%, p-0.02) was observed with TBI but no interaction was seen with other endpoints.
Conclusions
TBI based MAC resulted in significant reduction of NRM, translating into a better LFS without impacting aGVHD III-IV, chronic GVHD, RI or OS when compared to CT based MAC. Non-significant difference in OS between TBI and CT cohorts might be related to lower number of events, short follow-up and/or salvage therapies after relapse. These novel findings based on a large cohort of ALL patients, support the use of TBI based MAC and bone marrow graft in haplo-HCT with PTCy.
Dholaria:Celgene: Honoraria. Labopin:Jazz Pharmaceuticals: Honoraria. Angelucci:Novatis: Honoraria, Other: Chair Steering Committee TELESTO protocol; Celgene: Honoraria, Other: Participation in DMC; BlueBirdBio: Other: Local advisory board; Jazz Pharmaceuticals: Other: Local advisory board; Roche: Other: Local advisory board; Vertex Pharmaceuticals Incorp., and CRISPR Therapeutics: Other: Participation in DMC. Apperley:Bristol Myers Squibb: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Incyte: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Novartis: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau. Socie:Alexion: Consultancy. Mohty:Jazz Pharmaceuticals: Honoraria, Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal