

Introduction: Polycythemia vera (PV) is a myeloproliferative neoplasm (MPN) characterized by expansion of the granulocytic, erythrocytic, and megakaryocytic lineages in the bone marrow and peripheral blood, and in most cases, by the presence of a JAK2 mutation. Survival of patients with PV is decreased compared with age-matched controls, and this is mainly due to thromboembolic complications followed by progression to post-PV myelofibrosis and acute leukemia. While no curative treatment exists, cytoreductive treatment with hydroxyurea (HU) or ropeginterferon is approved in EU for first-line therapy, and ruxolitinib (RUX) is approved in EU and US for second-line therapy in patients with HU intolerance or resistance. The current futility analysis assesses the efficacy of ruxolitinib in newly-diagnosed PV treated within the Ruxo-BEAT trial.
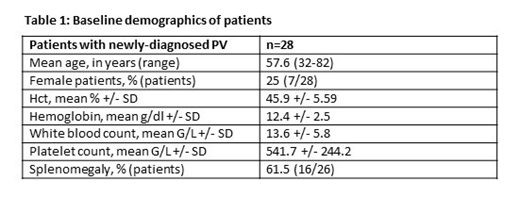
Methods: This clinical trial entitled "Ruxolitinib versus Best Available Therapy in patients with high-risk Polycythemia Vera or high-risk Essential Thrombocythemia" (Ruxo-BEAT; NCT02577926) is a multicenter, open-label, two-arm phase-IIb trial with a target population of 380 pts with PV and ET. Patients in first-line PV and in first and later lines ET are randomized in a 1:1 manner to receive either RUX or best available therapy (BAT). Crossover from BAT to RUX is possible in eligible patients after 6 months. Patients with PV in the RUX arm receive a starting dose of 10 mg bid and may increase their dose up to 20 mg bid. Primary endpoint is the rate of complete clinicohematologic response rate (CHR) at month 6 as defined by Barosi et al Blood 2009. Secondary endpoints include differences in the absence of phlebotomies, spleen size, patient-reported outcomes, and survival. This is a pre-specified futility analysis of RUX in the PV arm, after 50 PV patients had been enrolled. Of the 50 patients, 28 patients with newly-diagnosed PV were randomized into the RUX arm and were analyzed (a maximum of 6 weeks of HU, anagrelide, or interferon therapy was allowed). The PV arm would have to be closed if no favorable trend were observed for RUX for any of the following variables: (1) improvement (decrease) in the hematocrit level during 6 months of treatment, (2) improvement (decrease) of the JAK2V617F allele burden during 6 months of treatment, or (3) improvement of one of the following three symptom variables assessed by physician´s judgement or via MPN Symptom Assessment Form (MPN-SAF) during 6 months of treatment: pruritus, night sweats, or bone pain. Differences between screening (Hct) or baseline (all other variables) and end of month 6 (all variables) were calculated using Fisher´s exact test (for physician-assessed pruritus and night sweats) or the Wilcoxon matched-pairs signed rank test (all other variables).
Results: 28 patients received RUX for at least 6 months. After 6 months, the mean hematocrit level decreased from 45.9+/-5.6% to 41.0+/-5.0% (mean+/-SD) (p=0.0003). The number of phlebotomies calculated per year decreased from 4.2+/-3.9% to 0.96+/-2.1 (p=0.0009). Mean JAK2V617F allele burden decreased from 50.2+/28.4% to 44.0+/-28.5% (p=0.0039). The percentage of patients, as assessed by the physician, with pruritus or night sweats decreased from 41% to 26% (trending with p=0.13), and from 30% to 11% (p=0.02), respectively. The points reported by patients themselves on the MPN-SAF survey for pruritus decreased from 2.7+/-3.0 to 1.3+/-1.5 (p=0.0095) and there was a strong trend for reduction of night sweat points (from 3.1+/-3.6 to 1.6+/-2.4; p=0.0579), while the points for bone pain remained unaltered (2.0+/-2.8 to 1.4+/-2.2; p=0.215).
Conclusion: Treatment with ruxolitinib in first line PV is efficient regarding the above-mentioned endpoints. Recruitment of our trial will be ongoing. In order not to weaken the study´s statistical power, comparison of both arms was not performed.
Koschmieder:Ariad: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Bristol Myers-Squibb: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Incyte: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Shire: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis Foundation: Research Funding; CTI: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; AOP Pharma: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Bayer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees. Isfort:Mundipharma: Other: Travel reimbursement; Amgen: Other: Travel reimbursement; Hexal: Other: Travel reimbursement; BMS: Honoraria; Ariad: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria, Other: Travel reimbursement; Novartis: Consultancy, Honoraria, Other: Travel reimbursement; Roche: Other: Travel reimbursement; Alexion: Other: Travel reimbursement. Schafhausen:Novartis: Consultancy, Honoraria; Incyte: Consultancy, Equity Ownership, Honoraria. Griesshammer:Novartis: Consultancy, Honoraria, Speakers Bureau. Platzbecker:Abbvie: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria, Research Funding. Döhner:CTI Biopharma: Consultancy, Honoraria; Daiichi: Honoraria; Jazz: Honoraria; Novartis: Honoraria; Celgene: Honoraria; Janssen: Honoraria. Jost:Abbvie: Consultancy, Patents & Royalties: Royalty payments for the drug compound ABT-199, Research Funding; Bohringer: Consultancy, Research Funding; BMS: Consultancy, Speakers Bureau; Novartis: Consultancy, Speakers Bureau; Pfizer: Consultancy, Speakers Bureau; Celgene: Other: Travel Support; Novartis: Research Funding. von Bubnoff:Novartis: Research Funding. Stegelmann:Novartis: Consultancy, Honoraria; Incyte: Consultancy, Honoraria. Crysandt:Amgem: Other: travel grant; celgene: Other: travel grant; Pfizer: Other: travel grant; Gilead: Other: travel grant; Incyte: Membership on an entity's Board of Directors or advisory committees. Gezer:AMGEM: Membership on an entity's Board of Directors or advisory committees. Brümmendorf:Merck: Consultancy; Pfizer: Consultancy, Research Funding; University Hospital of the RWTH Aachen: Employment; Janssen: Consultancy; Ariad: Consultancy; Novartis: Consultancy, Research Funding.
Ruxolitinib as first-line treatment in newly-diagnosed PV

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal