

Background
Extranodal natural killer T cell lymphoma (ENKTL) is a rare subtype of non-Hodgkin lymphoma, of which pathogenesis is related to Epstein-Barr virus (EBV) infection. The presence of EBV-DNA in blood is a well-known prognosticator, which is also included in a prognostic model, PINK-E (Kim SJ et al, Lancet Oncol 2016). Furthermore, its presence after treatment is known to be a predictor of the treatment failure (Kim SJ et al, Lancet Haematol 2015). However, no consensus have been made on which blood sample (i.e, whole blood vs. plasma) is best to be used for the test. While EBV in plasma is known to have a higher specificity and sensitivity for EBV-related diseases as compared with EBV in peripheral blood mononuclear cells (Kanakry JA et al., Blood 2016), PINK-E model incorporated EBV status regardless of types of samples. We aimed to compare the prognostic performance of EBV DNA titers from whole blood (WB) and plasma.
Method
The EBV DNA viral load was measured in both WB and plasma samples by real-time quantitative PCR at the time of diagnosis, during and after completion of planned treatment. DNA was extracted using Artus® EBV RG PCR kit (Qiagen Inc.). The limit of detection level was 2.66 log copies/mL according to the manufacturer. Prognostic accuracy was compared by using time-dependent receiver operating characteristic (ROC) curves and corresponding area under the curve (AUC) values.
Results
A total of 60 patients with newly diagnosed ENKTL between September 2014 and September 2018 were included in this analysis. Twenty nine patients (48.3%) were in stage I, 6 (10.0%) in stage II, and 25 (41.7%) in stage IV. Forty six (76.7 %) patients had nasal involvement. Among them, 33 patients underwent concurrent chemoradiotherapy with weekly cisplatin and 53 received L-asparaginase containing chemotherapy (VIDL, n=46, 86.8%; SMILE, n=7, 13.2%) as definitive treatment or after chemoradiotherapy. Fifty two patients were evaluable for response: 33 (63.5%) complete response, 9 (17.3%) partial response, and 10 (19.2%) progressive disease. With a median follow-up duration of 34.1 months (range, 1.2-57.5 months), 2-year progression-free survival (PFS) and overall survival (OS) rates were 55.0% and 63.0%, respectively.
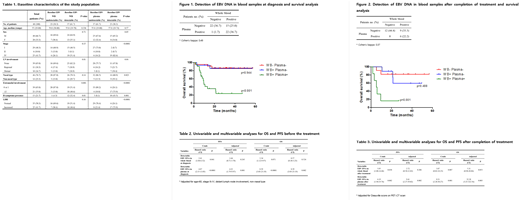
EBV-DNA was detected in 37 (61.7%) in pretreatment WB and 23 patients (38.3%) in plasma samples respectively (Table 1). There was moderate agreement (ƙ=0.49) between the tests. Discordant results were noted in 16 (26.7%) patients, 15 of whom were WB (+) and plasma (-). Presence of EBV DNA in plasma was significantly correlated with unfavorable clinical characteristics than that in WB (Table 1).
WB EBV positivity (2-year PFS rates, 42% vs 74%; HR 2.61, 95% CI, 1.04-6.52, p=0.041) and plasma EBV positivity (2-year PFS rates, 23% vs 75%; HR 4.87, 95% CI, 2.15-11.03, p<0.0001) were both associated with poor PFS. Plasma EBV positivity at diagnosis was a highly significant prognosticator of OS (2-year OS rates of 27% vs. 85%; HR 8.38, 95% CI, 3.03-23.19, p<0.0001). EBV status in the WB also tended to be associated with survival but without statistical significance (2-year OS rates, 47% vs 79%, HR 3.34, 95% CI, 1.12-9.96, P=0.071). Furthermore, WB EBV positivity in those with plasma EBV negativity was not prognostic for OS (2-year OS rates, 86% vs 84%, p=0.944) (Figure 1). On the other hand, plasma EBV status in those with WB EBV positivity was a significant predictor of OS (2yr OS rates, 84% vs. 29%, p<0.001). Multivariable analysis showed plasma EBV positivity was significantly association with poor PFS (HR 4.22, 95% CI, 1.79-9.97, p=0.001) and OS (HR 8.39, 95% CI, 3.03-23.19, p=0.002) (Table 2). The prognostic accuracy assessed by the time dependent ROC curve analysis for 2-year OS rates also showed higher AUCs with plasma than WB (0.79, 95% CI, 0.63-0.92 for plasma; 0.66, 95% CI, 0.37-0.81 for WB).
After completion of treatment, 22 patients were tested for EBV titer. Among those with plasma EBV positivity, WB EBV positivity was not associated with OS (2-year OS rates, 83% vs 62%, p=0.488). By contrast, plasma EBV positivity among those with WB EBV positivity was a significant predictor of OS (2yr OS rates, 62% vs. 17%, p=0.008) (Figure 2). In addition, post treatment plasma EBV DNA titer was a significant prognostic factors for PFS and OS by multivariable analysis (Table 3).
Conclusion
EBV DNA test in plasma is more accurate prognostic marker for ENKTL than that in WB as it can prognosticate regardless of EBV status in the WB.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal