

Background: Chronic lymphocytic leukemia (CLL) is one of the most common forms of adult leukemia in the Western population but rare in Chinese descent. As Chinese CLL patients have distinct clinical features, higher frequency of mutated IGHV as well as unique BCR stereotype, we hypothesize that genetic alterations may contribute to the disease phenotype differences. We profiled the known recurrent mutated genes associated with Western CLLs in 338 Chinese CLL samples, with the goal to define the somatic mutation pattern in the Chinese CLL population.
Methods: We first assessed 96 CLL mutated genes in a discovery cohort that includes 126 CLL samples using Illumina MiSeq platform. We then validated 20 recurrent mutated genes in a validation cohort that comprises of 212 CLL samples with Ion Torrent platform. The presence of mutation in DNA and mRNA were further validated by Sanger sequence.
Results: A total of 303 untreated and 35 relapsed samples were investigated. The average sequencing depth was 1957X (range: 112 to 4254). In the discovery cohort, we identified recurrently mutated genes in TP53 (17.5%), SF3B1 (14.3%), ATM (13.7%), KMT2D (12.7%), MYD88 (10.3%), NOTCH1 (8.7%), FBXW7 (8.7%), BIRC3 (7.9%), POT1 (4.8%), KRAS (4.0%). This was further confirmed in the validation cohort. In comparison to the frequency of these mutations in the western studies, we observed an unexpected significantly higher frequency of mutations in MYD88 and KMT2D (Chi-squared test, p<0.01).
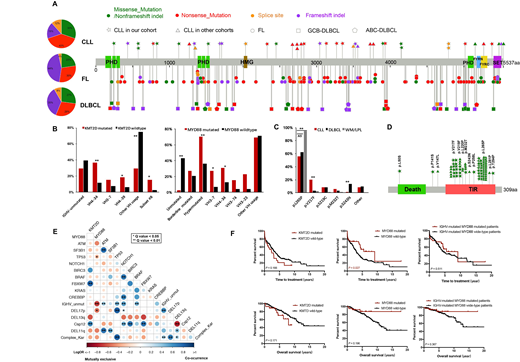
Mutations of KMT2D occurred with a similar frequency in treatment-naïve (8%) and relapsed samples (9%). 19/30 (63%) mutations were loss-of-function as they are predicted to generate truncated proteins due to lacking part or all of the C-terminal domains (Figure 1A). We observed a significant co-occurrence between KMT2D mutations and trisomy 12 (Chi-squared test, p<0.01, Figure 1E), suggesting there could be intrinsic linkage between these lesions. Further integration with IGHV mutation status revealed that CLLs with KMT2D mutations were characterized by an overrepresentation of VH4-34 and VH4-39 (p<0.01, p=0.03, respectively) and enriched in stereotyped subset #8 (4/12, 33.3%) (Figure 1B). Consistent with previous reports that VH4-34 and VH4-39 are commonly used in Asians CLLs, we confirmed the high frequency of subset #8 in Chinese patients [1], indicating KMT2D as a uniquely mutated gene in Chinese CLLs.
MYD88 mutations were found in 38/303 (13%) untreated CLLs. 17/38 (45%) of the mutations were at the L265P site (Figure 1C). Additional hotspot mutations were also detected (V217F 29%; S219C 13%). These mutations are associated with a significant male predominance (Chi-squared test, p<0.01), increased monoclonal gammopathy (15%, p=0.01), and a higher rate of Hepatitis B virus (HBV) infection (HBV core antibody positivity 56%, p=0.02). Most of these mutations (87%) were clonal and IGHV mutated (97%). It is worth to note that the usage of VH3-7 and VH4-34 were more dominant in patients with MYD88 V217F/S219C (6/16, 38%) and with L265P (6/17, 35%), respectively. Mutations of MYD88 are mutually exclusive with TP53 mutation and del(17p) (Chi-squared test, p<0.01). Moreover, we found a superior time to first treatment in MYD88-mutated patients compared with wide-type patients (Log-rank test, p=0.03).
To further understand the linkage between mutations and clinical outcome, we divided 303 treatment-naive patients into two groups: Non-progressor (NPRO, 39%) and Progressor (PRO, 61%). NPRO and PRO were classified as patients who developed symptoms that need treatment either more than or less than three years after sampling. Epigenetic modifiers pathway mutations (KMT2D, CREBBP, EP300, TET2, ARID1A and IKZF1) were more frequently in PRO group (17% vs. 8%, p=0.02). Inflammatory pathway mutations (MYD88, BIRC3, CARD11 and TRAF3) was more involved in NPRO group, compared to PRO or Relapsed samples (21%, 15% and 0%, p<0.01). Conversely, DNA damage pathway mutations (TP53, ATM and POT1) was more frequently found in Relapsed and PRO groups compared to NPRO group (49%, 30% and 7%, p<0.01).
Conclusion: In summary, we observed high frequency mutations in KMT2D and MYD88 that correlated with specific IGHV repertoire in Chinese CLL population. This suggests that pathogenesis of CLL between the Chinese and Western population may be different and potentially have therapeutic value.
[1] Marinelli M, et al. Oncotarget. 2016 Apr 12;7(15):20520-31.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal