


Increased expression of ERG (ETS-related gene), a proto-oncogene within the ETS (erythroblast transformation specific) family, is associated with an unfavorable clinical outcome in AML patients. A mechanism for ERG over-expression is ERG amplification. ERG amplification is present in 4-6% of adult AML. This study investigates the genetic profile of ERG-amplified AML by assessment of genomic copy number changes and mutational status of AML-related genes and how this correlates to treatment response and overall outcome. Currently copy number analysis is not recommended by ELN or WHO as a diagnostic standard in AML.
An institutional retrospective review of 205 adult AML cases from 2015 to 2018 provided two cohorts: a discovery cohort and control cohort. The discovery cohort includes 11 cases (4%) with ERG amplification. All cases in the discovery cohort include either TP53 mutation and/or loss/LOH of 17p. Thus, we developed a control cohort of 39 cases with TP53 abnormalities without ERG amplifications to determine the role TP53 plays in the observed outcomes. The 179 adult AML cases from the TCGA public database comprises the validation cohort, which incorporates both copy number and molecular sequencing data. Approximately 4% of AML cases in the TCGA dataset show ERG amplification.
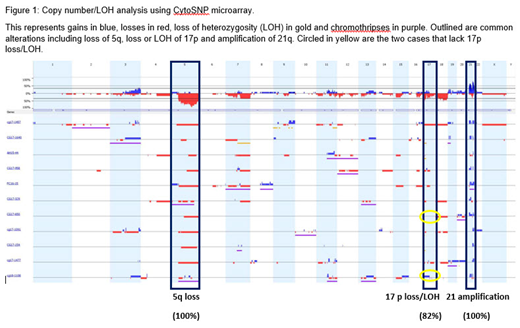
For our discovery and control cohorts, genomic DNA was extracted (Maxwell, Promega, Madison, WI) from fresh bone marrow aspirates. Copy number/LOH analysis was performed using the CytoSNP microarray (Illumina, San Diego, CA). Sequence variants were evaluated in hotspot regions of 49 genes using the ThunderBolts Myeloid Panel library preparation (RainDance Technologies, Billerica, MA) and paired-end sequencing (MiSeq, Illumina, San Diego, CA). Alignment and variant calling was performed with MiSeq Reporter (Illumina) and NextGene (Soft Genetics, State College, PA) and sequences were annotated using VarSeq (Golden Helix, Bozman, MT).
SNP microarray analysis of the discovery cohort revealed a distinct pattern of complex cytogenetics including chromothripsis, TP53 loss/LOH and loss of 5q. Molecular sequencing was available for 10 of 11 patients. All specimens analyzed for mutational status demonstrated TP53 loss of function mutations. The majority of cases (9/11) demonstrated complete loss of function of TP53 by mutation in conjunction with a "second hit" in the form of loss due to deletion or LOH of 17p. These nine patients failed to achieve any response with chemotherapy with a median survival time of 3.8 months. The two surviving patients had a single TP53 mutation with an intact second allele. Both of these patients are post-allogeneic stem cell transplant with no evidence of relapse.
There is an association of ERG amplification with MDS as 8 of the 11 patients transformed from very-high risk MDS. The interaction between ERG and TP53 allows one to predict treatment response and outcomes based on the presence or absence of an intact TP53 allele. Within the control group, there were no significant differences in survival or response to treatment based on number of intact TP53 alleles.
The validation cohort of TCGA patients confirmed the strong positive correlation between ERG amplification and TP53 mutations. There were 8 cases with ERG amplification. Of these, 6 cases had a similar genetic pattern found in the discovery cohort including TP53 mutations, loss of 5q and complex cytogenetics. The median overall survival (OS) of this cohort of ERG amplified + TP53 mutation was 2.5 months.
ERG amplification classifies a high-risk population of AML detected by copy number/LOH analysis with a distinct genetic signature including loss of 5q, complex cytogenetics including chromothripsis and loss of function TP53 mutation. The successive loss of the second TP53 allele in the setting of ERG amplification identifies a subset of patients with resistance to cytarabine and a very poor prognosis. These patients are unlikely to benefit from cytotoxic chemotherapy and may have improved outcomes with alternative regimens and/or clinical trial. ERG amplification is associated with AML that transforms from very-high risk MDS. Recognizing these patients before transforming to AML could allow for early transplant. This high-risk subgroup is currently un-recognized by standard cytogenetics and genetic mutation profiling; therefore, we recommend that copy number/LOH analysis become part of the standard diagnostic testing for MDS and AML.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal