

Background: BPDCN is a clinically aggressive myeloid malignancy that has historically demonstrated poor outcomes. Recent patho-biological observations have led to new therapies and improved outcomes, including the first approved therapy in the field with CD123-directed therapy (Pemmaraju et al. NEJM April 2019). BPDCN is recognized for its overexpression of CD123+/IL3Rα in 100% of cases (Frankel Blood 2014); BPDCN is also characterized by its BCL-2 overexpression (Montero Cancer Discovery 2017) and splicing factor and other molecular abnormalities commonly seen in MDS, CMML, and AML (Alayed Am J Hematol 2013). It is well known that patients (pts) with BPDCN can subsequently transform to AML. However, little is known about pts with BPDCN with prior/or concomitant hematologic malignancies (PCHM) and we therefore sought to determine pt characteristics and outcomes for this important subset of pts with BPDCN.
Patients: We analyzed all pts treated at our institution (1998-2019). 87 pts (83% male) were identified; n=57 untreated; n=27 prior therapy, with median number therapies = 1 [1-5]. Median age was 65 years [20-86 years]. Bone marrow (BM) was involved in 56 (64%), skin-only in 30 (34%), lymph node-only 1(1%). CD4+ and CD56+ were expressed in all pts tested; additionally, CD123+ and TCL-1+ was found in all pts tested. Cytogenetics were available in 74 pts: diploid (70%), complex (23%), deletion (12p13) (3%), miscellaneous (4%). Median BM blast count was 13% [0-95].
Frontline Therapies: a rapidly changing paradigm: Over time, a variety of treatments have been used in frontline setting: clinical trial/targeted therapy (including tagraxofusp) (n=29); HCVAD-based (including venetoclax) (n=27); other/miscellaneous regimens (n=13); CHOP (n=8); AML-based induction (n=5). hypomethylator-based (including venetoclax) (n=3); bortezomib-based (n=2). In the overall cohort (n=87), the median follow-up time was 15.5 months (mo) [4.3-65.4]. First complete remission (CR1) was achieved in 60%; median CR1 duration: 23.4 mo [1.5-155.6]. Median overall survival (OS) was 20.2 mo [1.0-158.0]. 67% of pts have died, with most common cause of death being sepsis/multi-organ failure.
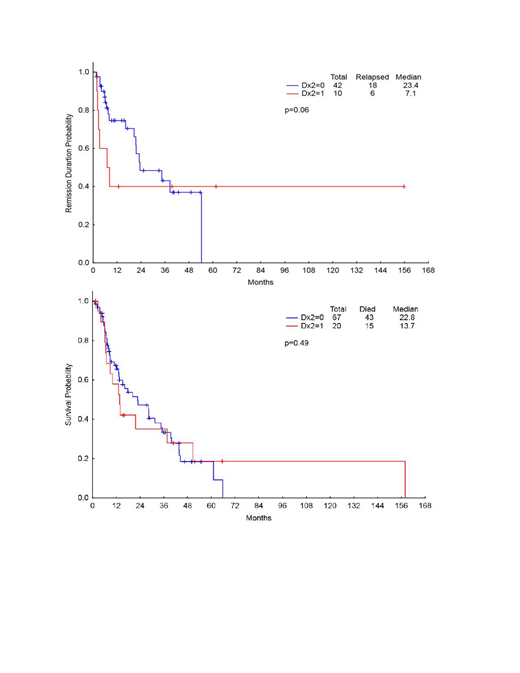
BPDCN with prior or concomitant hematologic malignancy (PCHM): Among the total BPDCN group (n=87), we found n=20 (23%) presented as BPDCN with PCHM. We compared these 20 pts with PCHM vs the remaining 67 pts without, and found no statistically significant differences between the two groups for baseline characteristics of age, sex, number of prior therapies or bone marrow blasts. Among BPDCN with PCHM cohort (n=20), breakdown of hematologic malignancy subtypes: MDS (n=9); CMML (n=5); myelofibrosis (n=3); lymphoid/myeloma (n=1 each: T-ALL, Hodgkin lymphoma, multiple myeloma). While there was no statistically significant difference found between the two groups for CR1 and OS, there was a trend towards significance for shorter CR1 in the BPDCN with PCHM group (p=0.06) (Figure).
Molecular Analysis: Among the total cohort, n=50 (57%) pts have been captured for next-generation sequencing (NGS) (n=34 without PCHM; n=16 with PCHM): the most common abnormalities were: TET2 mutation/variant (76%); ASXL1 (20%); RAS (11%). There was no statistically significant difference in terms of mutation patterns between BPDCN with PCHM and those without PCHM.
Conclusions: For the first time in our ongoing BPDCN clinic analysis, treatment with clinical trial has now become the most commonly employed therapeutic strategy for pts with BPDCN. In this new era of novel treatments, it is important to note that pts with BPDCN with PCHM are quite commonly encountered, most commonly with prior or concomitant MDS or CMML. Etiologies for this are multifactorial and will be an important area of research for the field, and will include further investigation of shared stem origin of these associated hematologic malignancies, older age of pts with BPDCN, and presence of CHIP, and/or myeloid mutation markers in many pts with BPDCN, including those with skin-only BPDCN. Because this entity of PCHM is so common in the BPDCN field, these pts should continue to be enrolled on all BPDCN clinical trials, and because this group may exhibit unique disease biology with trend towards shorter CR1, we propose the creation for a new category of BPDCN: BPDCN with PCHM.
Figure: (a): CR1 of Dx2=0 (no PCHM) vs Dx2=1 (has PCHM); Figure: (b): OS of Dx2=0 (no PCHM) vs Dx2=1 (has PCHM)
Pemmaraju:mustangbio: Consultancy, Research Funding; abbvie: Consultancy, Honoraria, Research Funding; samus: Research Funding; celgene: Consultancy, Honoraria; cellectis: Research Funding; Stemline Therapeutics: Consultancy, Honoraria, Research Funding; novartis: Consultancy, Research Funding; plexxikon: Research Funding; Daiichi-Sankyo: Research Funding; sagerstrong: Research Funding; affymetrix: Research Funding; incyte: Consultancy, Research Funding. Kantarjian:Daiichi-Sankyo: Research Funding; Amgen: Honoraria, Research Funding; Takeda: Honoraria; Jazz Pharma: Research Funding; Cyclacel: Research Funding; AbbVie: Honoraria, Research Funding; Immunogen: Research Funding; Agios: Honoraria, Research Funding; Novartis: Research Funding; BMS: Research Funding; Astex: Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Ariad: Research Funding; Pfizer: Honoraria, Research Funding. Khoury:Angle: Research Funding; Kiromic: Research Funding; Stemline Therapeutics: Research Funding. Loghavi:GLG Consultants: Consultancy; AlphaSights: Consultancy; MDACC: Employment. Cortes:Sun Pharma: Research Funding; Immunogen: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Merus: Consultancy, Honoraria, Research Funding; Daiichi Sankyo: Consultancy, Honoraria, Research Funding; Bristol-Myers Squibb: Consultancy, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Research Funding; Forma Therapeutics: Consultancy, Honoraria, Research Funding; Astellas Pharma: Consultancy, Honoraria, Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; BiolineRx: Consultancy; Biopath Holdings: Consultancy, Honoraria. Garcia-Manero:Amphivena: Consultancy, Research Funding; Helsinn: Research Funding; Novartis: Research Funding; AbbVie: Research Funding; Celgene: Consultancy, Research Funding; Astex: Consultancy, Research Funding; Onconova: Research Funding; H3 Biomedicine: Research Funding; Merck: Research Funding. Jabbour:BMS: Consultancy, Research Funding; Adaptive: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Cyclacel LTD: Research Funding; Takeda: Consultancy, Research Funding. Verstovsek:Incyte: Research Funding; Roche: Research Funding; NS Pharma: Research Funding; Celgene: Consultancy, Research Funding; Gilead: Research Funding; Promedior: Research Funding; CTI BioPharma Corp: Research Funding; Genetech: Research Funding; Blueprint Medicines Corp: Research Funding; Novartis: Consultancy, Research Funding; Sierra Oncology: Research Funding; Pharma Essentia: Research Funding; Astrazeneca: Research Funding; Ital Pharma: Research Funding; Protaganist Therapeutics: Research Funding; Constellation: Consultancy; Pragmatist: Consultancy. Jain:BMS: Research Funding; Pfizer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; ADC Therapeutics: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Incyte: Research Funding; AstraZeneca: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Servier: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Cellectis: Research Funding; Verastem: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Precision Biosciences: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Adaptive Biotechnologies: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pharmacyclics, an AbbVie company: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen Pharmaceuticals, Inc.: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; AbbVie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Genentech: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Qazilbash:Autolus: Consultancy; Bioclinical: Consultancy; Genzyme: Other: Speaker; Amgen: Consultancy, Other: Advisory Board.
Venetoclax is not fda approved for BPDCN, but based on our pre-clinical and clinical work , we have found activity in BPDCN

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal