


Background: Guadecitabine (G) is a next generation subcutaneous (SC) hypomethylating agent (HMA) resistant to degradation by cytidine deaminase which results in prolonged in vivo exposure to the active metabolite decitabine. We conducted a large global randomized phase 3 study of G vs Treatment Choice (TC) with azacitidine (AZA), decitabine (DEC), or low dose Ara-C (LDAC) in 815 TN AML patients unfit for IC (ASTRAL-1 study). The primary ITT results were previously presented (Fenaux et al, EHA abstract S879, 2019). Clinical guidelines for single agent HMAs recommend a minimum of 4 to 6 treatment cycles for maximum benefit. We describe here the results of the study based on number of treatment cycles administered.
Methods: TN-AML patients ineligible for IC due to age ≥ 75 y, or coexisting morbidities, or ECOG PS 2-3 were randomized 1:1 to either G (60 mg/m2/d SC for 5-days Q28 days) or a preselected TC of AZA, DEC, or LDAC at their standard dose/schedule. AML diagnosis and response status were assessed by an independent central pathologist blinded to randomization assignment. Complete response (CR) and overall survival (OS) were co-primary endpoints. We analyzed patients' characteristics, number of treatment cycles, reasons for treatment discontinuation, CR, and OS including analyses by number of cycles received including prospective subgroups, and OS analyses of responders and non-responders.
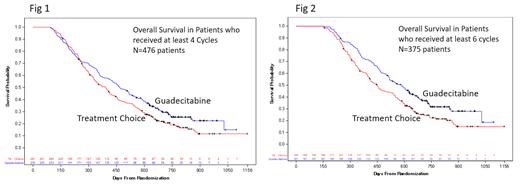
Results: 815 patients were randomized to G (408) or TC (407). Preselected TCs prior to randomization were DEC (43%), AZA (42%), and LDAC (15%). Baseline variables were well balanced across the 2 treatment arms. For G vs TC respectively, age ≥75 y in 62% vs 62.4%, PS 2-3 in 50.5% vs 50.4% (including 10.8% vs 8.8% PS 3), and poor risk cytogenetics in 34.3% vs 34.6%. Most patients were assigned to an HMA at randomization (759, 93%) with only 56 patients (7%) randomized to receive LDAC. Both CR (19.4% for G and 17.4% for TC), and OS Hazard Ratio (0.97; 95% CI 0.83-1.14) were similar and not significantly different between G and TC. Many patients in both arms did not receive the recommended minimum of 4 cycles (42.4% vs 40.8% for G vs TC respectively), or 6 cycles (54.2% vs 53.8% for G vs TC). The proportions were well balanced between the 2 treatment arms. Characteristics of patients who received at least 4 or 6 cycles were also well balanced between the 2 treatment arms for age, PS 2-3, secondary AML, poor risk cytogenetics, BM blasts >30%, and proliferative AML (total white cell count ≥20,000/uL). The primary reasons and proportions for treatment discontinuation were similar for the 2 treatments arms. For patients with <4 and <6 cycles respectively they are, in descending order, early deaths (16.7% and 20.7% of the overall ITT population), progression (7.6% and 11.7%), adverse events (5.8% and 6.9%), and patient decision (5.5% and 7.1%). In patients who received at least 4 cycles more patients achieved CR on G (33.6%) vs TC (28.6%), and median OS was longer on G (15.6 months for G vs 13 for TC, HR 0.78, 95% CI 0.64-0.96, log-rank p 0.02, Fig 1). Similarly, in patients who received at least 6 cycles, there were more CR on G (40.1%) vs TC (36.2%) and median OS was longer on G (19.5 months for G vs 15.0 for TC, HR 0.69, 95% CI 0.54-0.88, log-rank p 0.002, Fig 2). Subgroup analyses of OS in patients who received at least 4 or 6 cycles showed that survival benefit from G over TC was consistent in all prospective subgroups including against each of the 3 TCs (AZA, DEC, and LDAC). OS analyses in patients who received at least 4 or 6 cycles also favored G vs TC in both responders (CR, CRp, CRi, or PR) and non-responders with maximum benefit in patients who received at least 6 cycles (G vs TC OS HR 0.66, 95% CI 0.45-0.96, log-rank p 0.028 for responders, and HR of 0.73, 95% CI 0.53-1.00, log-rank p 0.048 for non-responders).
Summary/Conclusions: In a large global 815-patient randomized study of G vs TC composed mainly of first generation HMAs, G was at least as effective as TC based on the primary ITT analysis of CR and the narrow 95% CI of OS HR (0.83-1.14). Analyses of patients by number of treatment cycles showed that those who received at least 4 or 6 cycles achieved longer OS in G vs TC with the largest benefit in those who received at least 6 cycles. The benefit was observed in all subgroups, and in both responders and non-responders. Treatment with single agent guadecitabine should continue as long as the patient can still benefit and for at least 6 cycles to gain the maximum survival benefit.
Roboz:Trovagene: Consultancy, Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees; Sandoz: Consultancy, Membership on an entity's Board of Directors or advisory committees; AbbVie: Consultancy, Membership on an entity's Board of Directors or advisory committees; Actinium: Consultancy, Membership on an entity's Board of Directors or advisory committees; Agios: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amphivena: Consultancy, Membership on an entity's Board of Directors or advisory committees; Argenx: Consultancy, Membership on an entity's Board of Directors or advisory committees; Astex: Consultancy, Membership on an entity's Board of Directors or advisory committees; Astellas: Consultancy, Membership on an entity's Board of Directors or advisory committees; Bayer: Consultancy, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees; Celltrion: Consultancy, Membership on an entity's Board of Directors or advisory committees; Daiichi Sankyo: Consultancy, Membership on an entity's Board of Directors or advisory committees; Eisai: Consultancy, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees; Jazz: Consultancy, Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees; MEI Pharma: Consultancy, Membership on an entity's Board of Directors or advisory committees; Orsenix: Consultancy, Membership on an entity's Board of Directors or advisory committees; Otsuka: Consultancy, Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees; Roche/Genentech: Consultancy, Membership on an entity's Board of Directors or advisory committees. Döhner:Celgene, Novartis, Sunesis: Honoraria, Research Funding; AbbVie, Agios, Amgen, Astellas, Astex, Celator, Janssen, Jazz, Seattle Genetics: Consultancy, Honoraria; AROG, Bristol Myers Squibb, Pfizer: Research Funding. Mayer:AOP Orphan Pharmaceuticals AG: Research Funding. Krauter:Pfizer: Honoraria. Robak:Takeda: Consultancy, Research Funding; UCB: Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Other: Travel grant, Research Funding; Amgen: Consultancy, Other: Travel grant; Roche: Consultancy, Other: Travel grant, Research Funding; Abbvie: Consultancy, Honoraria, Other: Travel grant, Research Funding; Gilead: Consultancy, Research Funding; BeiGene: Consultancy, Research Funding; Acerta: Research Funding; Morphosys AG: Research Funding. Kantarjian:Agios: Honoraria, Research Funding; Astex: Research Funding; Jazz Pharma: Research Funding; Amgen: Honoraria, Research Funding; BMS: Research Funding; Novartis: Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Immunogen: Research Funding; AbbVie: Honoraria, Research Funding; Takeda: Honoraria; Cyclacel: Research Funding; Pfizer: Honoraria, Research Funding; Daiichi-Sankyo: Research Funding; Ariad: Research Funding. Novak:Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees; Roche: Consultancy, Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Other: Travel,Accommodations; Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees; Janssen: Other: Travel,Accommodations. Jedrzejczak:Takeda: Consultancy; Amgen: Consultancy, Other: travel support for hematology meetings; Celgene: Other: travel support for hematology meetings; Novartis: Research Funding; Roche: Other: travel support for hematology meetings. Thomas:PFIZER: Honoraria; ABBVIE: Honoraria; DAICHI: Honoraria; INCYTE: Honoraria. Miyazaki:Chugai: Research Funding; Otsuka: Honoraria; Novartis: Honoraria; Nippon-Shinyaku: Honoraria; Dainippon-Sumitomo: Honoraria; Kyowa-Kirin: Honoraria. Brandwein:Jazz Pharma: Consultancy, Honoraria; Otsuka: Honoraria; Pfizer: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Roche: Research Funding; Novartis: Consultancy, Honoraria. Demeter:Angelini: Other: Advisory Board; Pfizer: Other: Advisory Board; Novartis: Other: Advisory Board; Bristol Myers Squibb: Other: Advisory Board; Amicus: Other: Advisory Board; Amgen: Other: Advisory Board; Roche: Other: Advisory Board. Griffiths:Astex Phramaceuticals/Otsuka Pharmaceuticals: Consultancy, Research Funding; Persimmune: Consultancy; Persimmune: Consultancy; Genentech, Inc.: Research Funding; Appelis Pharmaceuticals: Other: PI on a clinical trial; New Link Genetics: Consultancy; Novartis Inc.: Consultancy; Novartis Inc.: Consultancy; Onconova Therapeutics: Other: PI on a clinical trial; Partner Therapeutics: Consultancy; Appelis Pharmaceuticals: Other: PI on a clinical trial; Boston Scientific: Consultancy; Boston Scientific: Consultancy; Genentech, Inc.: Research Funding; Abbvie, Inc.: Consultancy; Celgene, Inc: Consultancy, Research Funding; Celgene, Inc: Consultancy, Research Funding; New Link Genetics: Consultancy; Onconova Therapeutics: Other: PI on a clinical trial; Partner Therapeutics: Consultancy; Astex Phramaceuticals/Otsuka Pharmaceuticals: Consultancy, Research Funding; Abbvie, Inc.: Consultancy, PI on a clinical trial. Yee:Agensys, Astex, Hoffman La Roche, MedImmune, Merck, Millenium, Roche/Genentech: Research Funding; Novartis, Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; Astellas, Celgene, Otsuka, Shire, Takeda: Membership on an entity's Board of Directors or advisory committees. Hao:Astex Pharmaceuticals, Inc.: Employment. Azab:Astex Pharmaceuticals, Inc.: Employment. Fenaux:Celgene Corporation: Honoraria, Research Funding; Aprea: Research Funding; Astex: Honoraria, Research Funding; Jazz: Honoraria, Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal