

Background: Acquired thrombotic thrombocytopenic purpura (aTTP) is a rare, life-threatening autoimmune thrombotic microangiopathy that involves abnormal processing of von-Willebrand factor (vWF) and results in multiple organ dysfunction. Although aTTP remains a very unpredictable disease, risk factors for death include older age, lactate dehydrogenase (LDH) levels >10x the upper limit of normal (ULN), and cerebral involvement (i.e., the French severity score) (Benhamou et al. Haematologica 2012;97:1181-1186). In addition, raised cardiac troponin-I (cTnI) levels of >2.5 µg/L have also been linked with a higher risk of mortality or refractoriness (Benhamou et al. J Thromb Haemost 2015;13:293-302). In the randomized, double-blind, placebo-controlled phase 3 HERCULES study, patients with aTTP were randomized to placebo or caplacizumab, plus daily therapeutic plasma exchange and immunosuppression. This analysis aimed to determine the efficacy of caplacizumab in patients participating in HERCULES according to baseline disease severity.
Methods: In the HERCULES study, very severe disease was defined as:
a French severity score ≥3, or
severe neurological involvement (i.e. coma, seizures, focal deficit), or
cardiac involvement (cTnI >2.5xULN)
All of these factors have independently been associated with worse outcomes and higher mortality. The French severity score is a discrete score from 0 to 4, involving evaluation of 3 parameters:
Cerebral involvement: yes=1; no=0
LDH: >10xULN=1; ≤10xULN=0
Age: >60 years=2; >40 and ≤60 years=1; ≤40 years=0
Scores ≥3 indicate very severe disease.
Data from patients participating in HERCULES were extracted and analyzed according to less severe/very severe disease and are presented descriptively.
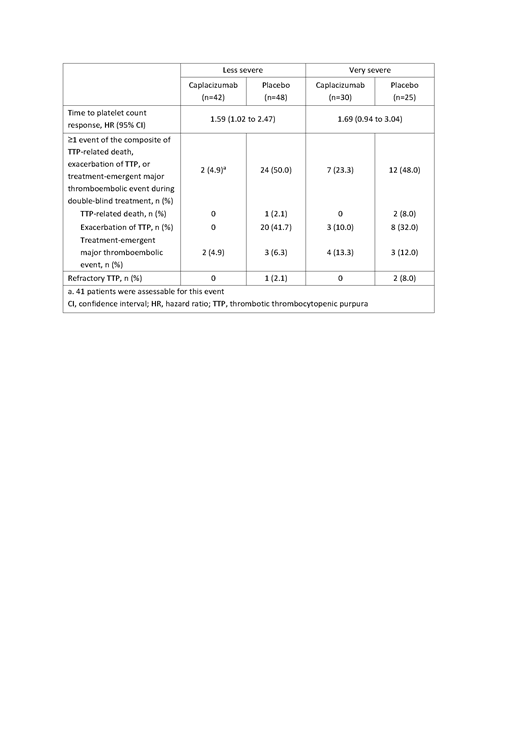
Results: Overall efficacy outcomes according to baseline disease severity are presented in Table 1. Patients who presented with less severe disease at baseline had a similar risk of mortality compared with patients who presented with very severe disease. Similar trends were observed for other clinically relevant outcomes, such as exacerbations of aTTP and refractoriness. Treatment with caplacizumab improved outcomes in both patient subgroups. Irrespective of disease severity, caplacizumab treatment resulted in faster platelet count normalization and a lower proportion of patients experiencing the composite endpoint of TTP-related death, exacerbation of TTP, or treatment-emergent major thromboembolic event during the double-blind treatment period. No patients who received caplacizumab died, while deaths occurred in 1 (2.1%) and 2 patients (8.0%) in the less severe and very severe subgroups of patients who received placebo, respectively. No patients receiving caplacizumab developed refractory disease, whereas 1 (2.1%) and 2 placebo-treated patients (8.0%) with less severe and very severe disease, respectively, developed refractory disease.
Conclusions: aTTP can be unpredictable, and, although this analysis included a small patient population, our results suggest that patients with less severe disease at baseline are equally at risk of death, refractoriness and exacerbations as patients with very severe disease. A clear treatment benefit was observed in all patients who received caplacizumab irrespective of disease severity at baseline, which highlights the importance of starting therapy early in all patients with aTTP.
Table 1. Overall efficacy outcomes according to baseline disease severity in the HERCULES study, during the double-blind treatment period.
Coppo:Shire: Consultancy; Alexion: Consultancy; Ablynx/Sanofi: Consultancy. Cataland:Ablynx/Sanofi: Consultancy, Research Funding; Alexion: Consultancy, Research Funding. Peyvandi:Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Sanofi: Membership on an entity's Board of Directors or advisory committees; Kedrion: Honoraria; Grifols: Honoraria; Alnylam: Honoraria; Bioverativ: Membership on an entity's Board of Directors or advisory committees; Octapharma: Research Funding. Knoebl:Ablynx/Sanofi: Consultancy; Novo-Nordisk: Consultancy, Research Funding; Shire/Takeda: Consultancy; CSL-Behring: Consultancy; Roche: Consultancy. Scully:Novartis: Consultancy; Shire: Research Funding; Alexion: Consultancy; Shire/Takeda: Consultancy; Ablynx/Sanofi: Consultancy. Kremer Hovinga:Ablynx/Sanofi: Consultancy, Honoraria, Other: Honoraria go to employer (Insel Gruppe AG, Department of Hematology); Roche: Honoraria, Other: Honoraria go to employer (Insel Gruppe AG, Department of Hematology); Shire: Consultancy, Other: Honoraria go to employer (Insel Gruppe AG, Department of Hematology), Research Funding; CSL-Behring: Honoraria, Other: Honoraria go to employer (Insel Gruppe AG, Department of Hematology); Siemens: Honoraria, Other: Honoraria go to employer (Insel Gruppe AG, Department of Hematology). Metjian:AblynxNV/Sanofi: Consultancy, Research Funding; Genentech: Consultancy, Research Funding. De La Rubia:Takeda: Consultancy; AMGEN: Consultancy; AbbVie: Consultancy; Janssen: Consultancy; Celgene Corporation: Consultancy. Pavenski:Shire: Honoraria; Alexion: Honoraria, Research Funding; Octapharma: Research Funding; Bioverativ: Research Funding; Ablynx: Honoraria, Research Funding. De Winter:Ablynx, a Sanofi company: Employment. de Passos Sousa:Sanofi: Employment. Callewaert:Sanofi (formerly employed by Ablynx, a Sanofi company): Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal