

Background: Observation is currently the standard of care for patients with smoldering and indolent multiple myeloma (MM). However, the evidence has been building up recently to support early initiation of treatment. We performed a meta-analysis of previous clinical trials involving smoldering/indolent MM patients who were treated with novel anti-myeloma agents to examine progression free survival (PFS) and safety profile of the treatment regimens.
Methods: A systematic literature search was conducted independently by 2 authors (F.C. and T.Z.K.) in PubMed, MEDLINE, EMBASE, Cochrane, and abstracts from major oncology meetings. Keywords used in the search included "myeloma", "smoldering MM", "indolent MM", "asymptomatic MM". The title and abstract of studies identified in the search were reviewed by 2 authors (F.C. and T.Z.K.) independently to exclude studies that were not clinical trials and included patients with MGUS or symptomatic MM. Entire text of the remaining articles, including the references, was examined to identify studies which reported Cox regression analysis for PFS or Kaplan-Meier curve of PFS to be able to extract HR, 95% CI, and P value, as previously described by Tierney JF et al. (Trials, 2007). Historical control arm is extracted from intermediate and high risk patients in an observational clinical trial by Khan R et al. (Haematologica, 2015) and used for the phase 2 clinical trials. The Jadad scale was used to assess the methodological quality of phase 3 trials. The random-effects model was used to synthesize the data. Heterogeneity was assessed using Cochran's Q statistic and I2 statistics, p≤0.1 and I2>50% considered statistically significant, respectively. We examined publication bias quantitatively using the Begg and Mazumdar adjusted rank correlation test and qualitatively by visual inspection of funnel plots of the logarithmic HR versus their standard errors.
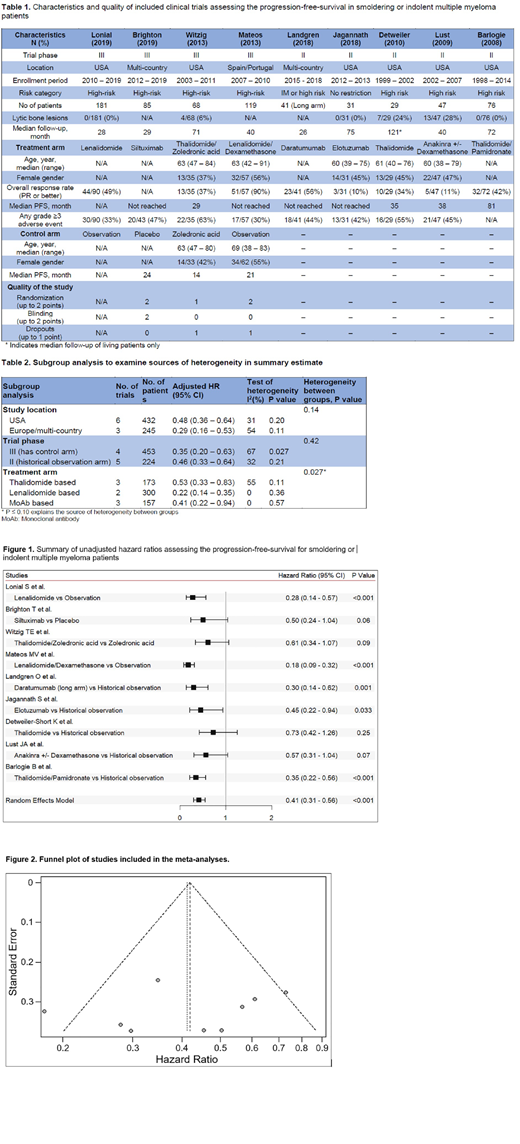
Results: We reviewed title/abstracts of 3327 studies, identified 31 manuscripts/meeting abstracts to read entire text, and incorporated 9 trials (four phase 3 and five phase 2) in the meta-analysis based on inclusion criteria. These studies cumulatively reported 677 patients with smoldering/indolent MM. Six trials were performed in USA, 2 were multi-country trials, and 1 was in Europe. Median number of patients in the trials was 68 (range: 29 - 181) and median follow-up was ranged between 26 and 121 months. The characteristics of these studies are shown in table 1.
Overall response rate and grade ≥3 adverse events for trials with thalidomide vs. lenalidomide vs. monoclonal antibody based treatment arms were 41% and 59% vs. 65% and 32% vs. 36% vs 44%. On meta-analyses of all studies, treatment vs observation of smoldering/indolent MM was statistically significant predictor of PFS (HR 0.41, 95% CI: 0.31 - 0.56, p < 0.001) (Figure 1). The results showed considerable heterogeneity (Cochran's Q test P = 0.037, I2 = 51%). There was no evidence of publication bias both quantitatively (P = 0.30) and on visual inspection of the funnel plot (Figure 2). We performed preplanned stratified analysis of studies based on location, trial phase, and treatment arm (Table 2). Subgroup analyses according to treatment regimens identified the trials with thalidomide based treatment arms as the source of heterogeneity (I2 = 55% vs I2 = 0%, P = 0.027). Trials with lenalidomide and monoclonal antibody based treatment arms showed significantly greater prognostic impact on PFS (HR 0.22, 95% CI: 0.14 - 0.35 and HR 0.41, 95% CI: 0.22 - 0.94, respectively) compared to trials with thalidomide based treatment arms (HR 0.53, 95% CI: 0.33 - 0.83).
Conclusion: In this first meta-analysis of patients with smoldering/indolent MM, we found that novel anti-myeloma agents prolongs the PFS with an acceptable toxicity profile.
Malek:Amgen: Speakers Bureau; Adaptive: Consultancy; Janssen: Speakers Bureau; Medpacto: Research Funding; Sanofi: Consultancy; Takeda: Consultancy; Celgene: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal