

Introduction: Pyruvate kinase (PK) deficiency causes a defect in the glycolytic pathway, leading to a hereditary hemolytic anemia. Management is supportive and consists of splenectomy, transfusions, and chelation therapy.
Aim: To better understand the comorbidity and complication profile of adults with PK deficiency, and the extent to which transfusion frequency contributes, the objectives of this study were to (1) quantify the prevalence of comorbidities and complications according to transfusion history and (2) compare the types and rates of select comorbidities and complications with the general population.
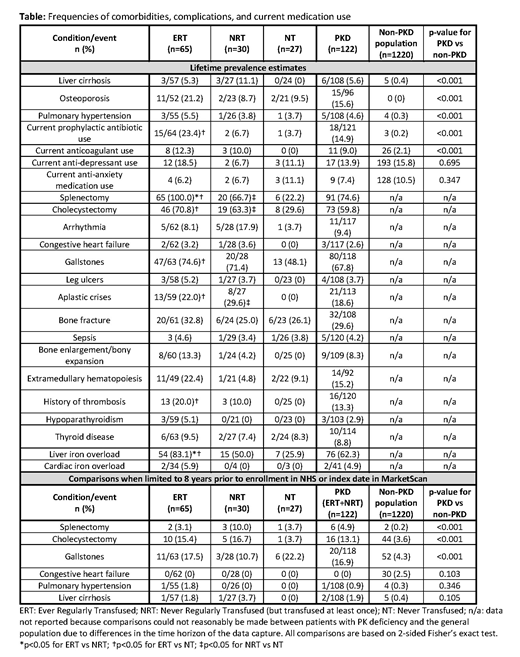
Methods: Data were obtained from the enrollment survey of the PK Deficiency Natural History Study (NHS), a longitudinal, retrospective and prospective cohort study in which clinical, laboratory, transfusion, and radiologic data were collected; all participants were confirmed to have 2 mutations in the PKLR gene. Patients (n=122) were eligible for this analysis if they were ≥18 years of age and had sufficient data on transfusion history to enable classification into 1 of 3 cohorts: "Ever Regularly Transfused" (ERT, defined as ≥6 transfusions in any 12-month period), "Never Regularly Transfused" (NRT, defined as having ≥1 lifetime transfusion but never having >4 transfusions in any 12-month period), or "Never Transfused" (NT). To contextualize the findings, the frequencies of select conditions were compared with an age- and gender-matched cohort of individuals from the insured, general US population who did not have any hemolytic anemia diagnoses and had ≥5 years of continuous enrollment in the Truven MarketScan administrative claims database. The NHS reported lifetime prevalence rates, whereas rates obtained from the MarketScan data were based on diagnosis and procedure codes over varying look-back periods; therefore, to minimize bias, we limited PK deficiency vs. general population comparisons to (1) chronic conditions that require lifetime management and would thus still be recorded in claims data years after initial diagnosis, and/or (2) conditions for which a diagnosis/procedure date was available in the NHS and could be matched in time to the average 8-year look-back period for the general population. Frequencies were compared across mutually exclusive cohorts using Fisher's exact 2-tailed tests of significance.
Results: ERT (n=65), NRT (n=30), and NT patients (n=27) had a mean age of 34.2, 39.5, and 37.2 years at enrollment, respectively (not significant [ns]), with 46.2%, 56.7%, and 59.3%, respectively, being male (ns). ERT patients trended toward being more likely than NT patients to be Amish and have the homozygous R479H splice variant (30.8% vs 11.1% [p=0.064]) but were significantly less likely to have a missense/missense PKLR genotype (32.3% vs 70.4% [p=0.001]). Compared with the general population, patients with PK deficiency had significantly higher rates of splenectomy, cholecystectomy, osteoporosis, liver cirrhosis, pulmonary hypertension, and current prophylactic antibiotic and anticoagulant use (Table). Rates of splenectomy, cholecystectomy, and osteoporosis were significantly higher in patients with PK deficiency, regardless of transfusion cohort, and both ERT and NRT patients had significantly higher rates of liver cirrhosis than individuals from the general population. A gradient was seen across transfusion cohorts for other conditions. Notably, 83.1% of ERT patients, 50.0% of NRT patients, and 25.9% of NT patients had a history of liver iron overload. ERT patients were also significantly more likely than NRT and NT patients to have had a splenectomy, cholecystectomy, and/or thrombosis, and to currently use prophylactic antibiotics. Findings were consistent when the analysis was restricted to non-Amish patients with PK deficiency.
Conclusions: Patients with PK deficiency have higher rates of select comorbidities and complications than age- and gender-matched individuals who do not have PK deficiency. Even patients with PK deficiency who have never been transfused are at increased risk of complications of the disease and its treatment.
Boscoe:Agios Pharmaceuticals, Inc.: Employment, Equity Ownership. Yan:Agios Pharmaceuticals, Inc.: Consultancy. Hedgeman:IBM Watson Health: Employment. van Beers:Agios Pharmaceuticals, Inc.: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Consultancy, Research Funding; Pfizer: Research Funding; RR Mechatronics: Research Funding. Al-Samkari:Agios: Consultancy, Research Funding; Dova: Consultancy, Research Funding; Moderna: Consultancy. Barcellini:Incyte: Consultancy; Alexion: Consultancy, Speakers Bureau; Agios Pharmaceuticals, Inc.: Consultancy; Novartis: Speakers Bureau; Apellis: Consultancy; bioverativ: Consultancy. Eber:Agios Pharmaceuticals, Inc.: Consultancy. Glader:Agios Pharmaceuticals, Inc: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding. Chonat:Alexion: Other: advisory board; Agios Pharmaceuticals, Inc.: Other: advisory board. Rothman:Agios: Honoraria, Research Funding; Novartis: Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding. Kuo:Agios: Consultancy; Alexion: Consultancy, Honoraria; Apellis: Consultancy; Bioverativ: Other: Data Safety Monitoring Board; Bluebird Bio: Consultancy; Celgene: Consultancy; Novartis: Consultancy, Honoraria; Pfizer: Consultancy. Kwiatkowski:Agios: Consultancy; bluebird bio, Inc.: Consultancy, Research Funding; Imara: Consultancy; Apopharma: Research Funding; Novartis: Research Funding; Celgene: Consultancy; Terumo: Research Funding. Ravindranath:Agios Pharmaceuticals, Inc.: Other: I am site PI on several Agios-sponsored studies, Research Funding. Neufeld:Octapharma, Shire Pharmaceuticals (Baxalta), Novo Nordisk, Celgene, NHLBI/NIH: Research Funding; Octapharma, Agios, Acceleron, Grifols, Pfizer, CSL Behring, Shire Pharmaceuticals (Baxalta), Novo Nordisk, ApoPharma, Genentech, Novartis, Bayer Healthcare: Consultancy; Octapharma: Other: study investigator, NuProtect study (Octapharma-sponsored). Holzhauer:Agios Pharmaceuticals, Inc.: Consultancy. Verhovsek:Sickle Cell Disease Association of Canada: Membership on an entity's Board of Directors or advisory committees, Research Funding; Canadian Haemoglobinopathy Association: Membership on an entity's Board of Directors or advisory committees; Vertex: Consultancy; Sickle Cell Awareness Group of Ontario: Membership on an entity's Board of Directors or advisory committees. Kunz:Novartis: Membership on an entity's Board of Directors or advisory committees. Sheth:Apopharma: Other: Clinical trial DSMB; Celgene: Consultancy; CRSPR/Vertex: Other: Clinical Trial Steering committee. Despotovic:Novartis: Research Funding; Dova: Honoraria. Grace:Agios Pharmaceuticals, Inc: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal