

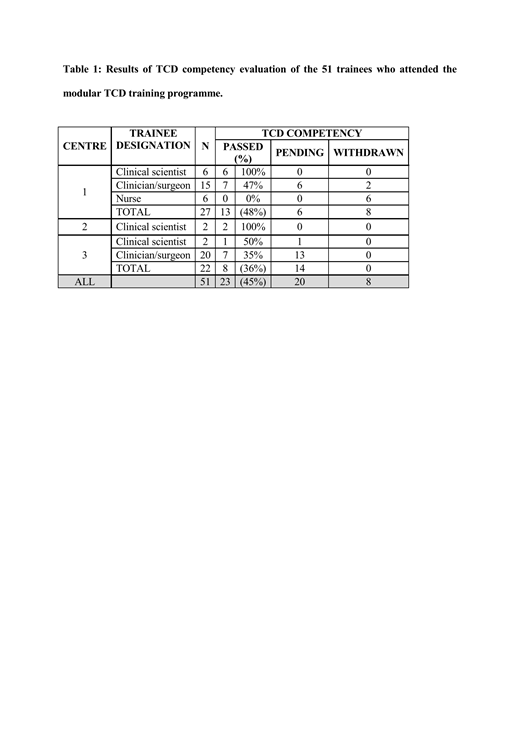
Background: Recent studies on the impact of migration on the geographical distribution of the HbS allele have highlighted sickle cell disease (SCD) as a global public health issue. Although considered a "rare disease" due to its global frequency in the 28 countries of the European Union, SCD is the most common genetic disease in France and the United Kingdom and its frequency is steadily rising in many other countries of central and southern Europe. At present, less than 50% of children with SCD have access to TCD screening in the USA and Europe. Most centers use the non-imaging approach, as described in the STOP trials, which is a "blind technique" where there is no guiding anatomical information and thus relies heavily on operator experience. Some centers now use imaging TCD which provides anatomical information enabling the Circle of Willis to be visualized and so facilitates identification of the basal cerebral arteries and orientation of the Doppler beam when acquiring blood velocities. The primary study objective was to determine the effectiveness of the modular training program in achieving the high level of scanning competency described in the STOP trial, irrespective of practitioner background and when using either non-imaging or imaging TCD. Methodology. The modular TCD training program was developed at the training center in London and delivered to trainees at all three centers (London-UK, Padova-Italy and Dublin, Ireland). The program comprised of a 2-day instructional course covering theory and practical aspects of TCD and incorporated significant hands-on instruction. This was followed by trainees scanning at their own hospital until they had collected a log book of at least 40 scans (within a one year period), after which a scan review and competency evaluation was performed. Results.Modular training program.Nine training courses were held (six in England, one in Ireland and two in Italy); these were attended by a total of 51 trainees (Table 1). Approximately half the trainees (45%) successfully completed the competency evaluation, 20 were still in training, two of whom had failed the assessment and eight withdrew from the program due to problems with local funding for staff or equipment. The ten trainees with an ultrasound background (clinical scientists) were able to acquire TCD skills rapidly as demonstrated by the high pass rate. The findings were more variable in the clinician group (pediatricians and nurses) with five requiring refresher courses and twelve failing to complete the minimum annual scan number (forty) due to small local sickle populations. Comparative analysis of TCD data obtained before and after training.A total of 555 patients were included in this study; 181 patients at Center 1 (52 males, mean age 7.9±3.8 (range 2-15.4 years), genotypes: 134 HbSS, 39 HbSC, 8 HbSβ thalassemia), 194 patients. Center 2 (53 males, mean age 7.4±3·2 (range 2-15.1 years), genotypes: 158 HbSS, 32 HbSC, 4 HbSβ) and 154 patients at Center 3 (50 males, mean age 6.4±3.5 (range 2-15.1 years), genotypes: 154 HbSS, 10HbSC, 16 HbSβ thalassemia). There was no significant difference in gender distribution (Chi-Square=0.313, p=0.85), but more young patients were recruited in Center 3 (ANOVA, F=8.9, p<0.001), more HbSC patients in Centers 1 and 2 and more Sβ thalassemia patients in Center 3 (Chi-Square=21.0, p<0.001).Conclusion: Diagnostic vascular ultrasound is highly operator-dependent; hence training and competency validation are essential in producing skilled TCD operators. The modular training program described here was effective in ensuring standardized TCD technique, irrespective of professional background. In this multi-center study TCD velocity measurements and STOP classification were consistent, irrespective of TCD mode and European country. We believe that this is the first modular training program that has demonstrated efficacy when delivered in different European countries. Delivery of this program in areas where TCD is under-provided will augment the number of trained TCD operators, thus facilitating access to specialist diagnostic services. This will have a significant impact on public health across Europe where SCD patients are increasing due to migration. Competency and quality assurance (QA) are important components of such a screening program; further work is in progress to develop an achievable QA program for ongoing regulation of this screening program.
Colombatti:AddMedica: Consultancy; Novartis: Consultancy; Global Blood Therapeutics: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal