

Patients with Sickle Cell Disease (SCD) frequently present for emergency care with pain or fever. The rate of emergency visits/year is between 2-4 per patient every year with 12% of patients visiting the emergency 4 or more times/year1. National medical organizations in Canada and the United States recommend pain therapy within 30 minutes of arriving to the emergency department2,3.
Feedback from patients in Canada reflected a lack of awareness of the medical community regarding the disease and optimal management. As a response Canadian Haemoglobinopathy Association2 (CanHaem), created the "Sickle Cell Disease Emergency Wallet Cards" which were inspired from the successful Hemophilia "Factor First Card4". The goal of the cards was to provide simple care instructions to an emergency responder and facilitate timely care for patients in crisis. These wallet cards have recommendations for treatment of pain and fever within 30 minutes, patient's diagnosis, program contact details, and patient's individual pain plan. The cards have been in circulation for 4 years. The purpose of this study was to determine if the cards are used by parents and patients as intended.
Research Questions:
1.Are the CanHaem Cards used by patients and families?
2. Do patients find the card helpful in facilitating their care delivery?
Methods: The surveys were administered to patients and/or proxies. Prior to survey distribution three parents/patients have verified the utility of the questions, the content and the readability of the survey. The survey was translated into French/Arabic by two independent translators per language. It was distributed in Alberta and British Columbia, Canada in specialty clinics known to use the cards. The University of Alberta Ethics Board deemed the project a quality improvement initiative and the ARECCI tool: A pRoject Ethics Community Consensus Initiative was completed prior to quality improvement project start.
Results: 140/184 participants completed the survey. The response rate: 76%. Demographics: 91% province of Alberta. Proxy: 49%; Patients: 51%. The majority of respondents were female: 54%, median age: 37 years (range 16-84 years).
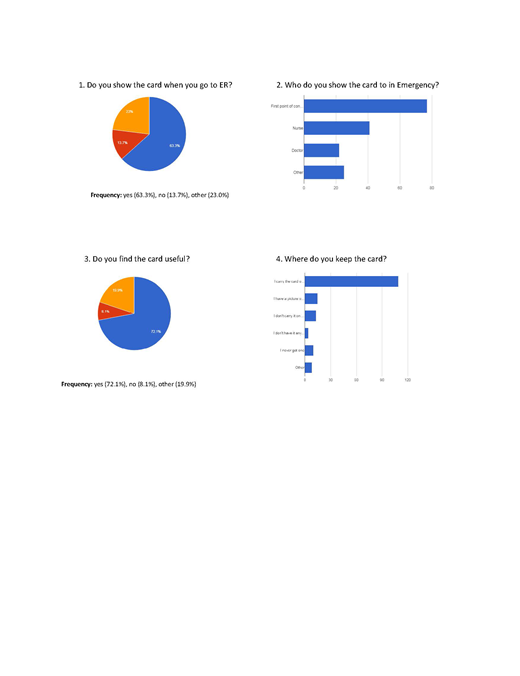
See graphs 1-4 below: 72.3% felt the card was helpful in their care. 78.6% carry the physical card (purse, wallet, and diaper bag), while 10.7% have a picture on their phone, 9.3% don't carry the card, 7.1% state they never received a card. The majority (63.6%) show the card at first contact in emergency, 48.9% felt staff read the card.
Total of 68 comments. 67.6% of comments were positive: "Sense of security"; "Get us in to see the doctor faster..." Neutral comments (22%) ranged from requests for lamination to provider response to the card being variable "sometimes it is faster and sometime(s) doesn't really change anything". Finally, 10% were negative reflecting long wait times "Good concept, the idea itself is great. Execution... could be improved greatly", and requests for more information on the card.
Conclusion: In Canada, SCD is an uncommon disease and many healthcare providers may not be aware of national and international guidelines regarding acute presentations. To help facilitate knowledge transfer and to aid communication with emergency services, CanHaem created wallet cards as a Canada-wide initiative. This survey demonstrates the patient/parent perspective of the emergency cards. Eighty-nine percent of patients/proxies carried the card (either digitally or physically) and 63% showed the card in the acute care setting. The discrepancy between those who carry the card and those who show it may reflect that numerous respondents stated they had not required emergency care since receiving the card as well some respondents were "carried away by the pain and forget to use the card". Comments revealed a sense of security and patient's appreciation for having the card available to them indicating the value of card to patients. The card demonstrates a simple and low cost intervention to facilitate emergency care for hemoglobinopathy patients.
References:
1. Paulukonis ST et al. Emergency department utilization by Californians with sickle cell disease. Ped Blood and Ca 2017. doi: 1002/pbc.26390
2. CanHaem https://www.canhaem.org/healthcare-professionals/
3. Evidence-Based Management of Sickle Cell Disease: Expert Panel, 2014.
4. Canadian Hemophilia Society. Stop the Bleeding. https://www.hemophilia.ca/files/ER%20CARD%20E_%20Jan%2009.pdf
Ezzat:Novartis: Honoraria, Speakers Bureau; ApoPharma: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal