

Introduction:
Allogeneic hematopoietic cell transplantation (allo-HCT) is a potentially curative therapy for high risk hematological diseases and sustained engraftment of the donor stem cells is essential for transplant success. Graft failure (GF) is a rare, but serious complication post allo-HCT. In the presented study we aimed to assess the incidence, risk factors in a single-center population and as well the impact on transplant outcome.
Methods:
Between 01 January 2015 and 31 December 2018, 557 patients underwent allo-HCT at our center. Data was collected retrospectively and updated in June 2019. Cases were included regardless of the underlying diagnosis, disease status prior to transplant, preparative regimen, or stem cell source. Primary graft failure was defined as failure to achieve an absolute neutrophil count (ANC) of >500/ µL by 28 days after bone marrow (BM) or peripheral blood stem cell (PB) transplantation. In contrast, secondary graft failure was defined as cytopenias after initial engraftment (ANC <500/µL), with (a) donor chimerism of less than 5% or (b) falling donor chimerism with intervention such as second transplant or donor lymphocyte infusion (DLI) or (c) patient death due to cytopenias, and fall in donor chimerism, even if chimerism was >5%. Exclusion criteria for diagnosis of GF were (a) disease relapse (b) graft versus host disease or (c) other causes of cytopenias such as, viral infections, or drug induced. Outcomes examined included overall survival (OS), cumulative incidence of GF, non-relapse mortality (NRM) and cause of death.
Results:
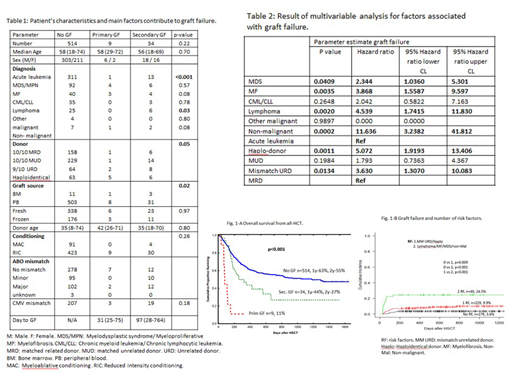
Baseline characteristics are summarized in (Table 1). GF was seen in 43 (7.7%) patients. Of these 43 patients, 9 (21%) had primary GF, and 34 (79%) had secondary GF. The cumulative incidence of GF overall (primary and secondary) is 1.6% (0.8- 3.0%) at day 100 and 6.5% (4.5-8.8%) at day 800. The median survival of patients following primary GF was 41 days versus 144 days in secondary GF. At one hundred days OS in primary GF was 22% and in secondary GF was 64%. The 1y and 2y OS for secondary GF was 33% and 28% respectively (Figure 1-A).
Multivariable analysis demonstrated that the (a) diagnosis/transplant indication (MDS, myelofibrosis, lymphoma or non-malignant diseases) and (b) donor type (HLA-mismatched unrelated or haploidentical) were the only factors significantly associated with increased GF (Table 2).
We determined the effect of more than one of these risk factors on the occurrence of graft failure as seen in (Figure 1-B). In the absence of any of the risk factors, the incidence of GF was 3.6%. If one risk factor was present, the incidence of GF was 9.9%, and if 2 risk factors were present, the incidence of GF was 24.5%.
In primary GF, 5 patients underwent second allo-HCT. In secondary GF, 15 patients (44%) underwent a second allo-HCT and another 8 patients received donor lymphocyte infusion. All the patients with primary GF died because of graft failure and its associated complications. In secondary GF, 22 patients (51%) died, 30% of causes related to infections.
Conclusions:
Our study showed an increased risk for graft failure following the use of mismatched unrelated or haploidentical donors for diseases such as lymphoma, myelofibrosis, myelodysplastic syndrome and non-malignant diseases. As well, we found that a presence of two risk factors puts patients at clinically significant increased risk of graft failure. More intense conditioning therapy should be considered for patients with one but in particular two risk factors.
Michelis:CSL Behring: Other: Financial Support.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal