

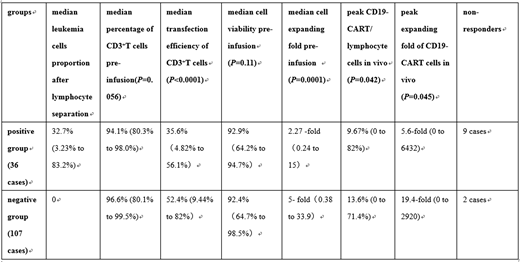
Introduction: Recently, chimeric antigen receptor (CAR) T-cell (CART) targeting CD19 has resulted in high complete remission (CR) rate in patients with refractory or relapsed B cell acute lymphoblastic leukemia (r/r B-ALL). Our previous clinical study has achieved more than 90% CR rate with CD19-CART in r/r B-ALL, but approximately 10% of patients have failed even CD19 high expression on their leukemia cells (Pan J, et al. Leukemia 2017; 31: 2587-2593). In current study, we investigate whether leukemia burden in peripheral blood (PB) has any influence in CART preparation ex vivo and its clinical efficacy. Patients and Methods: From June 2017 to June 2019, 143 r/r B-ALL patients received CD19-CART therapy. The median age was 8 years old (10 months to 65 years old). Thirty-six patients had leukemia cells in PB (positive group) and the median leukemia cells proportion after lymphocyte separation was 32.7% (3.23% to 83.2%); 107 patients had no leukemia cells detectable in PB (negative group). After apheresis, peripheral blood mononuclear cells (PBMCs) were isolated using lymphocyte separation liquid and leukemia cells proportion were determined by flow cytometry (FCM). PBMCs were activated with CD3 and CD28 antibodies for 24 hours, then transduced with the lentivirus encoding anti-CD19-CD3zeta-4-1BB CAR and cultured for 4-6 days in serum-free media containing IL2, IL7, IL15, IL21. Mycoplasma, endotoxin, bacteria and fungi were strictly controlled during the culture. Cell viability, expanding fold, percentage of CD3+ T cells, transduction efficiency and B cells were all examined before CART infusion. The patients received cyclophosphamide (250 mg/m2) and fludarabine (30 mg/m2) all for 3 days, and followed by CART infusion with a median number of 4.7 (0.6 to 43) X 105cells/kg. CD19-CART cells' expansion capacity in vivo was analyzed by FCM. Clinical efficacy was evaluated by bone marrow morphology and FCM on day 30. Results: Both normal B cells and leukemia B cells were all undetectable in infused CD19-CART. The median percentage of CD3+ T cells and transduction efficiency in positive and negative groups were 94.1% (80.3% to 98.0%) vs. 96.6% (80.1% to 99.5%) (P=0.056), and 35.6% (4.82% to 56.1%) vs. 52.4% (9.44% to 82%) (P<0.0001), respectively. The median cell viability and expanding fold in positive and negative groups were 92.9% (64.2% to 94.7%) vs. 92.4% (64.7% to 98.5%) (P=0.11), and 2.27-fold (0.24 to 15) vs. 5-fold (0.38 to 33.9) (P=0.0001), respectively. Post CD19-CART infusion, the median peak CD19-CART/ lymphocyte cells and peak expanding fold in vivo in positive and negative groups were 9.67% (0 to 82%) vs.13.6% (0 to 71.4%) (P=0.042), and 5.6-fold (0 to 6432) vs.19.4-fold (0 to 2920) (P=0.045), respectively. It was noteworthy that 6/9 non-responders in positive group and 1/2 non-responder in negative group had no detectable CD19-CART cell expansion in PB. On day 30 post CD19-CART infusion, 132/143 (92.3%) patients achieved CR or CR with incomplete count recovery (CRi). Nine of 36 (25%) patients in positive group and 2 of 107 (1.87%) patients in negative group had no response to CD19-CART therapy. Conclusions: Our study has shown that both normal B cells and leukemia B cells have been killed by CART cells during culture, which indicated good killing function of CD19-CART cells in our culture system. Our data have showed that leukemia burden in PB has resulted in not only much lower transduction efficiency of CD3+ T cells and cell expanding fold ex vivo, but also much lower peak CD19-CART and expanding fold in vivo, which has translated into poorer response to CD19-CART therapy. Therefore, reducing leukemia burden in PB before CART preparation is suggested to improve clinical efficacy.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal