

Background: Relapse occurs in 30-40% of AML patients undergoing allogeneic hematopoietic stem cell transplantation (alloHSCT). Detecting molecular relapse before clinical relapse offers the opportunity of early interventions (e.g. donor lymphocyte infusions, reduction of immunosuppression etc.). Next-generation sequencing (NGS)-based error-corrected sequencing approaches have shown promising results in AML patients prior to alloHSCT, which identified MRD in 45% of patients and predicted a cumulative incidence of relapse of 66% versus 17% in MRD negative patients at 5 years. However, NGS-based MRD is not well studied in patients after alloHSCT.
Aim: To evaluate the prognostic impact of MRD on day 90 and day 180 after alloHSCT in AML patients in morphologic complete remission (CR) using error-corrected NGS applicable to the majority of AML patients.
Patients and Methods: We quantified MRD in 138 patients who underwent myeloablative (MA, n=47) or reduced-intensity conditioned (RIC, n=91) alloHSCT for AML on day 90 and 180 after alloHSCT. All patients had at least one mutation at the time of diagnosis that was identified by NGS with a myeloid panel on the Illumina platform. Amplicon-based error-corrected sequencing and bioinformatics analysis was applied to samples on day 90 (n=133) and day 180 (n=125) after alloHSCT as described previously (Thol et al. Blood 2018). In the first approach we analysed 1-2 diagnostic mutations (=limited marker approach). In the second approach an extended marker set with (2-4) markers was used (=extended marker approach). Genomic DNA from peripheral blood (PB) was used for the majority of analyses (PB n= 394; bone marrow n=17). Cumulative incidence of relapse (CIR) and non-relapse mortality (NRM) were evaluated by competing risk analysis.
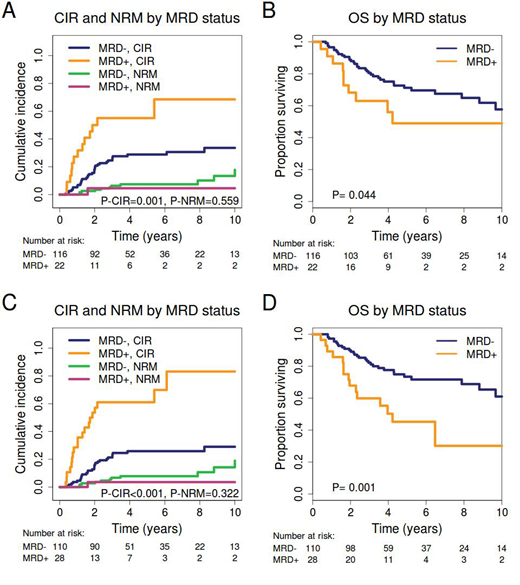
Results: The median follow up time of the cohort was 5.5 years. The mean limit of detection was a variant allele frequency (VAF) of 0.012% using error correction and 0.071 when using forward/reverse read error correction. MRD positivity on day 90 and/or day 180 was detected in 22 out of 138 patients (16%) with the limited marker approach, while MRD was found in 28 patients (20.3%) with the extended marker approach. Using the limited marker approach, the 5-year CIR was 52% for MRD positive and 30% for MRD negative patients (P=0.001), while NRM was similar between both groups (Figure 1A). Overall survival (OS) was shorter in MRD positive patients compared to MRD negative patients (P=.044, Figure 1B). In multivariate analysis using variables significant in univariate analysis (P<0.1), MRD remained significant for CIR (HR 3.19; CI 1.73-5.89; P<0.001). Using the extended marker approach improved the prognostic power with a 5-year CIR of 58% for MRD positive and 27% for MRD negative patients (P<0.001, Figure 1C) and reduced OS in MRD positive patients (P=0.001 Figure 1D) which remained significant in multivariate analysis for CIR (HR 4.75; CI 2.66-8.50; P=<0.001) and OS (HR 2.56; CI 1.26-5.20; P<0.009).
On day 90 after alloHSCT, 26 of 133 (20%) MRD positive patients were identified with the extended marker approach, while only 2 additional MRD positive patients were identified on day 180. 9 of 26 MRD positive patients on day 90 never relapsed during the follow up period. The rate of chronic GvHD was 29% in these patients compared to 43% in MRD negative patients (P=.28). MRD was detected in 17% of patients with acute graft-versus-host-disease (aGvHD) of any grade compared to 25% in patients with no aGvHD (P=0.23). To better understand which markers may be most useful for MRD analysis we sequenced 34 available samples at relapse. In 25 patients (74%), at least one mutation persisted from diagnosis to relapse and at least one mutation was gained at relapse. Eight patients (24%) had no overlapping mutation while only one patient had no change in the molecular profile between diagnosis and relapse.
Conclusion: NGS-based MRD monitoring on day 90 and 180 after alloHSCT is predictive for CIR and OS in AML patients. The discriminative power can be further improved when selecting 2-4 markers instead of a limited marker approach with only 1 to 2 markers per patient. Our results suggest that MRD from peripheral blood collected already at day 90 is prognostic for relapse and OS. Thus, day 90 NGS-based MRD monitoring from peripheral blood may become useful as a tool to tailor post-transplant care in AML patients.
Chaturvedi:Bayer Pharma AG, Berlin, Germany: Research Funding. Paschka:Agios: Membership on an entity's Board of Directors or advisory committees; Sunesis: Membership on an entity's Board of Directors or advisory committees; Amgen: Other: Travel expenses; Pfizer: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Takeda: Other: Travel expenses; BMS: Other: Travel expenses, Speakers Bureau; Abbvie: Other: Travel expenses; Astellas: Membership on an entity's Board of Directors or advisory committees; Astex: Membership on an entity's Board of Directors or advisory committees, Travel expenses; Otsuka: Membership on an entity's Board of Directors or advisory committees; Janssen: Other: Travel expenses; Novartis: Membership on an entity's Board of Directors or advisory committees, Other: Travel expenses, Speakers Bureau; Celgene: Membership on an entity's Board of Directors or advisory committees, Other: Travel expenses, Speakers Bureau; Jazz: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Bullinger:Menarini: Honoraria; Novartis: Honoraria; Pfizer: Honoraria; Sanofi: Honoraria; Seattle Genetics: Honoraria; Bayer: Other: Financing of scientific research; Hexal: Honoraria; Janssen: Honoraria; Abbvie: Honoraria; Amgen: Honoraria; Astellas: Honoraria; Bristol-Myers Squibb: Honoraria; Celgene: Honoraria; Daiichi Sankyo: Honoraria; Gilead: Honoraria; Jazz Pharmaceuticals: Honoraria. Fiedler:Amgen, Jazz Pharmaceuticals, Daiichi Sanchyo Oncology, Servier: Other: Support for meeting attendance; Amgen, Pfizer, Abbvie: Other: Support in medical writing; Amgen, Pfizer, Novartis, Jazz Pharmaceuticals, Ariad/Incyte: Membership on an entity's Board of Directors or advisory committees; Amgen: Research Funding. Krauter:Pfizer: Honoraria. Döhner:Daiichi: Honoraria; Jazz: Honoraria; Novartis: Honoraria; Celgene: Honoraria; Janssen: Honoraria; CTI Biopharma: Consultancy, Honoraria. Döhner:AROG, Bristol Myers Squibb, Pfizer: Research Funding; Celgene, Novartis, Sunesis: Honoraria, Research Funding; AbbVie, Agios, Amgen, Astellas, Astex, Celator, Janssen, Jazz, Seattle Genetics: Consultancy, Honoraria. Heuser:Bayer Pharma AG, Berlin: Research Funding; Synimmune: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal