

Introduction: Daratumumab, a CD38-directed monoclonal antibody, in combination with lenalidomide and dexamethasone (D-Rd), recently received FDA approval for the treatment of patients with newly diagnosed multiple myeloma (NDMM) ineligible for autologous stem cell transplantation (ASCT). FDA approval was based on results of the prespecified interim analysis of a pivotal phase III trial (MAIA) in which D-Rd was compared to Rd among patients with NDMM who were ineligible for ASCT. In the MAIA trial, D-Rd significantly reduced the risk of progression or death compared to Rd. However, no trials have compared D-Rd to other standard-of-care (SOC) regimens. The present study compared progression-free survival (PFS) of D-Rd from the MAIA trial database to common SOC regimens from the Flatiron Health EHR Database, a de-identified nationwide US database of records primarily from community-based oncology practices.
Methods: Patient-level data were obtained from the MAIA trial and the Flatiron database. Patients in the MAIA trial were enrolled between March 2015 and January 2017. To be included in MAIA, patients had to be deemed ineligible for high-dose chemotherapy with ASCT due to either age (≥65 years) or presence of comorbidities, have Eastern Cooperative Oncology Group performance status (ECOG PS) ≤2, creatinine clearance ≥30mL/min, and adequate bone marrow reserve.
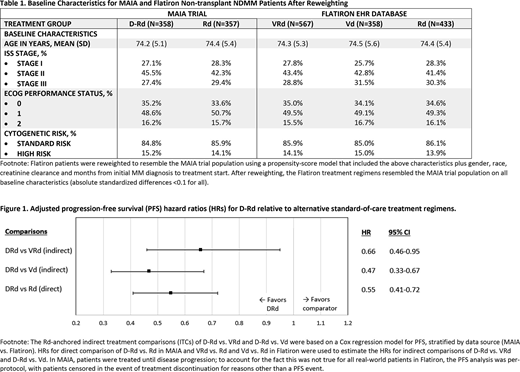
In the Flatiron Database, patients had to be diagnosed with MM between January 2011 and April 2019, age ≥65 years at initiation of first line treatment (LOT1), could not have received stem cell transplant as part of LOT1, and met MAIA inclusion/exclusion criteria. Regimens received by fewer than 10% of patients in Flatiron were excluded due to sample size and statistical power considerations. Bortezomib-lenalidomide-dexamethasone (VRd), bortezomib-dexamethasone (Vd), and Rd were the most commonly used regimens in non-transplant NDMM patients, representing 67% of regimens used in this setting. Multiple imputation by chained equations was used to address missing data in Flatiron. Eligible Flatiron patients treated with VRd, Vd, or Rd as LOT1 were reweighted to resemble the MAIA trial population on measured baseline characteristics using propensity-score (PS) weighting.
An anchored adjusted indirect treatment comparison (ITC) was performed to compare D-Rd to VRd and D-Rd to Vd, using a stratified Cox proportional hazards regression model with Rd as the common anchor across both data sources. The model calculates hazard ratios (HRs) for direct comparisons within MAIA (D-Rd vs Rd) and within Flatiron (VRd vs. Rd, Vd vs. Rd) to estimate the HRs indirectly for D-Rd vs. VRd and D-Rd vs. Vd.
Results: After application of MAIA inclusion criteria and PS-reweighting, the Flatiron VRd, Rd, and Vd patients resembled the MAIA trial population on baseline patient demographics and clinical characteristics (Table 1). D-Rd statistically significantly reduced the risk of progression or death compared to Rd (HR=0.55; 95% CI, 0.41-0.72) based on the direct comparison with D-Rd using the MAIA trial data; D-Rd statistically significantly reduced the risk of progression or death compared to VRd (HR=0.66; 95% CI, 0.46-0.95) and Vd (HR=0.47; 95% CI, 0.33-0.67) based on the anchored ITC (Figure 1).
Sensitivity analyses will be performed and updated analysis using longer follow-up data from the MAIA study will be presented at the meeting.
Conclusion: This analysis demonstrated that D-Rd reduced the risk of progression or death compared to other SOCs VRd and Vd for patients with NDMM who are transplant-ineligible. In the absence of head-to-head trials, this type of patient-level analysis provides important information that can help optimize treatment for patients with NDMM who are transplant-ineligible.
Durie:Amgen, Celgene, Johnson & Johnson, and Takeda: Consultancy. Kumar:Takeda: Research Funding; Janssen: Consultancy, Research Funding; Celgene: Consultancy, Research Funding. Usmani:Amgen, Celgene, Janssen, Sanofi, Takeda: Speakers Bureau; Amgen Array Biopharma, Bristol-Myers Squibb, Celgene, Janssen, Merck, Pharmacyclics, Sanofi, Takeda: Other: Research Grant; Amgen, Bristol-Myers Squibb, Celgene, Janssen, Merck, SkylineDX, Takeda: Other: Consultant/Advisor. Ammann:Janssen: Employment, Equity Ownership. Lam:Janssen: Employment, Equity Ownership. Kobos:Janssen: Employment. Maiese:Janssen: Employment, Equity Ownership. Facon:Celgene: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Takeda: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Amgen: Membership on an entity's Board of Directors or advisory committees; Sanofi: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal