


Background: AML is an aggressive malignancy with a median age of 67 yrs at diagnosis and an age-adjusted 5-yr survival of less than 25%. Most older patients (pts) with AML have poor risk cytogenetic/genetic features associated with suboptimal complete remission (CR) rates and overall survival (OS). Until recently, the anthracycline and cytarabine based induction remained unchanged for over 4 decades. Vosaroxin (Vos) is a first-in-class anticancer quinolone derivative which is thought to induce less cardiac toxicity than standard anthracycline therapy. Vos was previously administered in combination with intermediate dose cytarabine (IDAC) in relapsed/refractory (r/r) AML pts in a large randomized phase 3 trial (VALOR) and demonstrated significantly improved CR rates compared to IDAC alone but without improvement in OS. In the VITAL study, we investigated the combination of infusional cytarabine (iAC) with Vos ("7 + V") in newly diagnosed AML.
Methods: VITAL (NCT02658487) is a single-arm, open-label, two-stage phase II study of 90 mg/m2, Vos on days 1 and 4 (reduced to 70 mg/m2, days 1 and 4 in the event of re-induction) and 100 mg/m2 continuous iAC on days 1-7. Oral cryotherapy was administered during Vos administration as prophylaxis for oral mucositis seen in prior studies. Enrollment in stage 1 was limited to 17 evaluable pts >55 yrs of any risk classification or pts 18-54 years with high-risk disease. The two-stage design required CR in more than 7 of the first 17 pts in order to proceed to stage 2. The operating characteristics of the study design provided a 64% probability of early termination if CR occurred in 7 or fewer pts suggesting that the true CR rate would be ≤ 40%. Stage 2 included an additional 24 pts (age 18-54 yrs with intermediate or high-risk disease, or 55 years or older with any risk disease). Response was assessed using the modified IWG-2003 criteria.
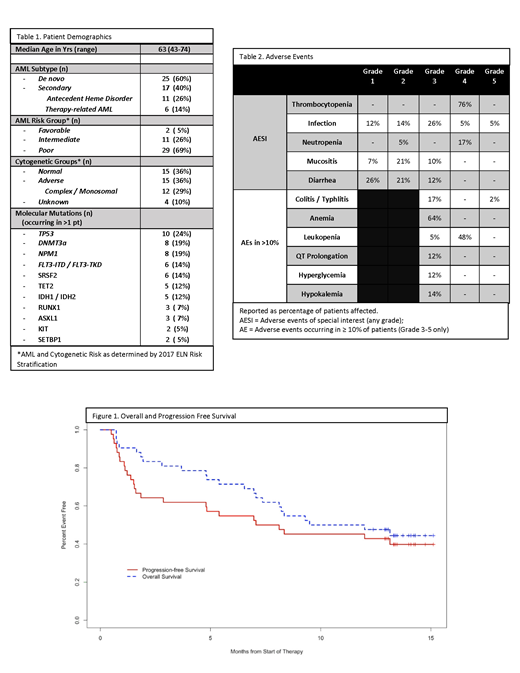
Results: In total, 42 pts were enrolled and assessed for toxicity. One patient who achieved an aplastic marrow biopsy at day 14, succumbed to an AML-related sepsis event prior to formal response assessment was initially deemed unevaluable for response and replaced but was ultimately included in the response assessment. Baseline demographics of the 42 enrolled pts are seen in Table 1a. Median age was 63 yrs (range, 43-74) and 86% (36/42) were ≥ 55yrs at time of enrollment. Almost all, 40/42 (95%), had intermediate (11/40) or poor (29/40) risk AML. Adverse events (AEs) of special interest of any Grade (Gr) and Gr 3-5 AEs occurring in > 10% of pts are listed in Table 1b. Oral mucositis was observed in 16/42 (38%) pts with 12/42 (29%) having Gr 1-2 and only 4/42 (10%) having Gr 3 severity. Three Gr 5 events occurred (2-Infection/Sepsis; 1-neutropenic colitis). No acute cardiac toxicity was seen. CR was achieved in 20/42 (48%) pts, while 3 additional pts achieved CR with incomplete count recovery (CRi) for a CR/CRi rate of 55% (23/42). CR was observed in 100% (2/2) with favorable risk (both >65 yrs old). CR/CRi was seen in 73% (8/11) intermediate and 45% (13/29) poor risk pts. One poor risk pt with CRi converted to CR in the absence of additional therapy but did so outside of the protocol defined time period for response assessment (Day 57 +/- 3 days) and was recorded as CRi for this analysis. CR/CRi was noted in 40% (4/10) pts whose AML had TP53 mutations. Allogeneic hematopoietic stem cell transplant was performed in 45% (19/42) of pts. Progression-free survival was 43% and OS was 48% for all pts at 1-year of follow-up (Figure 1).
Conclusion: The combination of Vos and iAC in newly diagnosed AML pts appears safe. Mucocutaneous complications were observed as noted in previous studies with Vos. Administration of oral cryotherapy during Vos administration appeared to reduce occurrence of oral mucositis during induction, but > Gr 3 neutropenic enterocolitis occurred in 7/42 (17%) pts. Still, the combination appears to be tolerable with an adverse event profile analogous to conventional induction regimens. While the VALOR trial observed Gr 3-5 cardiac AEs in < 1% of the 705 r/r AML pts with prior anthracycline exposure, no attributable cardiac events were seen within the VITAL trial population. Vosaroxin and infusional cytarabine is a clinically active induction regimen which warrants further investigation based on response rates and toxicity profile at least similar to current anthracycline based induction strategies with an apparent absence of cardiac toxicity.
Strickland:Astellas: Consultancy; Jazz: Consultancy; Kite: Consultancy; Pfizer: Consultancy; Novartis: Consultancy; Sunesis: Research Funding; AbbVie: Consultancy. Podoltsev:Alexion: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Agios Pharmaceuticals: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Blueprint Medicines: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Incyte: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Boehringer Ingelheim: Research Funding; Kartos Therapeutics: Research Funding; Astellas Pharma: Research Funding; Daiichi Sankyo: Research Funding; Sunesis Pharmaceuticals: Research Funding; Jazz Pharmaceuticals: Research Funding; Pfizer: Research Funding; Astex Pharmaceuticals: Research Funding; CTI Biopharma: Research Funding; Celgene: Other: Grant funding, Research Funding; Genentech: Research Funding; AI Therapeutics: Research Funding; Samus Therapeutics: Research Funding; Arog Pharmaceuticals: Research Funding. Zeidan:Acceleron Pharma: Consultancy, Honoraria, Research Funding; Celgene Corporation: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy, Honoraria, Research Funding; Otsuka: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Medimmune/AstraZeneca: Research Funding; Boehringer-Ingelheim: Consultancy, Honoraria, Research Funding; Trovagene: Consultancy, Honoraria, Research Funding; Incyte: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; ADC Therapeutics: Research Funding; Jazz: Honoraria; Ariad: Honoraria; Agios: Honoraria; Novartis: Honoraria; Astellas: Honoraria; Daiichi Sankyo: Honoraria; Cardinal Health: Honoraria; Seattle Genetics: Honoraria; BeyondSpring: Honoraria. Byrne:Karyopharm: Research Funding. Gore:Celgene Corporation: Consultancy, Research Funding. Savona:Celgene Corporation: Membership on an entity's Board of Directors or advisory committees; Boehringer Ingelheim: Patents & Royalties; AbbVie: Membership on an entity's Board of Directors or advisory committees; Sunesis: Research Funding; TG Therapeutics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding; Selvita: Membership on an entity's Board of Directors or advisory committees; Karyopharm Therapeutics: Consultancy, Equity Ownership, Membership on an entity's Board of Directors or advisory committees; Incyte Corporation: Membership on an entity's Board of Directors or advisory committees, Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal