

BACKGROUND. B-cell receptor (BCR) signaling is a central driver for chronic lymphocytic leukemia (CLL), and its targeting through irreversible inhibition of Bruton's tyrosine kinase (BTK) by ibrutinib has significantly improved the prognosis of CLL patients. Ibrutinib treatment has become standard of care, and, recently, has advanced to the first-line setting. A treatment-induced, sometimes dramatic increase of peripheral lymphocytosis, has emerged as a class effect of BTK inhibitors in CLL. Mechanistically, BTK blocking by ibrutinib might affect adhesion molecules and chemokine receptors, such as CXCR4 and CXCR5, thus interfering with the protective tissue microenvironment and mobilizing tissue-resident CLL cells from the lymph nodes and bone marrow into the peripheral blood. This hypostasized mechanism of a "compartment shift," however, has not yet been demonstrated experimentally or visually. Positron emission tomography (PET) with [68Ga]Pentixafor, a radiotracer that specifically targets the CXCR4 receptor, was recently established as a sensitive approach with which to detect CLL in vivo. As a proof-of-concept, we here present three CLL patients to demonstrate the potential of [68Ga]Pentixafor-PET/MR imaging to functionally track CLL cells along the redistribution induced by ibrutinib.
METHODS. Three CLL patients were included: patient 1 was a 74-year-old treatment-naïve male, with unmutated IGHV status and high-risk cytogenetics, including del17p13 and TP-53 mutation; patient 2 was a 53-year-old female with late relapse (12 years after allogeneic stem cell transplantation), IGHV was unmutated, and cytogenetic abnormalities included del11q22 and del13q14; and patient 3 was a 59-year-old treatment-naïve male with unmutated IGHV and del11q22 and del13q14. Whole-body PET/MRI with injection of 150 MBq of [68Ga]Pentixafor was performed pre and on ibrutinib treatment (patient 1: one week; patient 2: two weeks; and patient 3: three weeks after start of the first therapy cycle, respectively). Treatment consisted of continuous oral administration of 420 mg of ibrutinib. Mean standardized [68Ga]Pentixafor uptake values (SUVmean) of involved lymph nodes, the bone marrow, and the spleen were measured. Isolated peripheral blood mononuclear cells (PBMCs) were stained with fluorescence-labeled antibodies, and measurements were performed on flow cytometer.
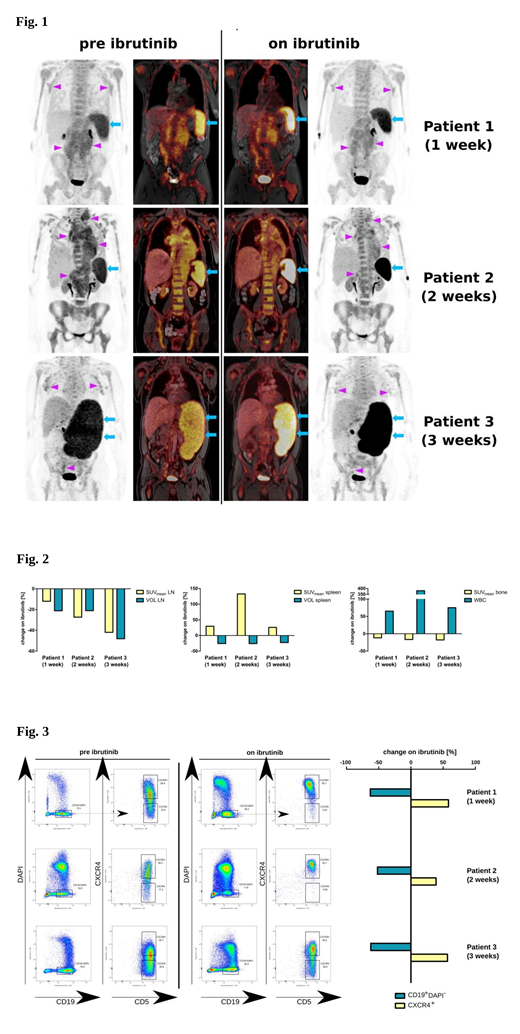
RESULTS. In all three cases - at one week, two weeks, and three weeks on ibrutinib treatment - CXCR4 density, as measured on [68Ga]Pentixafor-PET, shifted from the bone marrow and lymph nodes toward the spleen (Figs. 1-3). In patient 1, the SUVmean decreased in the bone marrow (-9.8%) and lymph nodes (-12.0%), whereas it increased markedly in the spleen (+29.8%). At flow cytometry, this patient exhibited an increase of CXCR4-high (tissue-resident) CLL cells upon ibrutinib treatment (+56.7% relative to baseline). In patient 2, the SUVmean decreased in the bone marrow (-14.7%) and lymph nodes (-27.3%), whereas it more than doubled in the spleen (+133.0%). At flow cytometry, individual CLL cells demonstrated a relative increase (+39.1%) of CXCR4 positivity. In patients 3, the SUVmean decreased in the bone marrow (-27.6% %) and lymph nodes (-41.9%), whereas it increased markedly in the spleen (+26.1%). At flow cytometry, the relative increase of CXCR4-high CLL cells was +58.3%.
CONCLUSIONS. We here provide the first pictures of the early functional treatment effects of ibrutinib. While our analyses confirmed a shift of CXCR4 positive CLL cells from lymph nodes to peripheral blood, they also revealed that ibrutinib rapidly released CLL cells from the bone marrow. Also, unexpectedly, CLL cells redistributed to the orthotopic splenic cavernous system. Visualization of CLL on ibrutinib supports the pre-existing clinical hypothesis of a "compartment shift", however it also modified and refined the mechanistic model by describing early clearing of the bone marrow and re-distribution to the peripheral blood and the spleen.
Jaeger:Celgene, Roche, Janssen, Gilead, Novartis, MSD, AbbVie, Sanofi: Membership on an entity's Board of Directors or advisory committees; Novartis, Roche, Sandoz: Consultancy; AbbVie, Celgene, Gilead, Novartis, Roche, Takeda Millennium: Research Funding; Amgen, AbbVie, Celgene, Eisai, Gilead, Janssen, Novartis, Roche, Takeda Millennium, MSD, BMS, Sanofi: Honoraria. Wester:Scintomics: Other: Spouse CEO of Company; CXCR4-targeted radiopharmaceuticals: Other: Inventor; Scintomics GmbH, Germany: Other: Shareholder. Staber:AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; MSD: Honoraria, Speakers Bureau; Takeda-Millenium: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Janssen: Honoraria, Speakers Bureau; Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal