

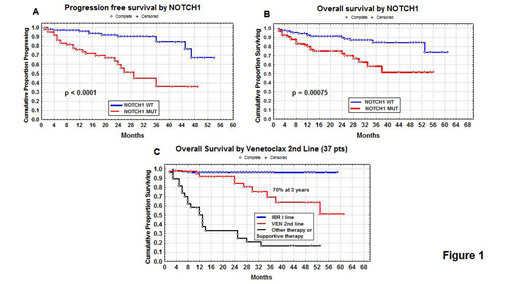
The advent of agents inhibiting the BCR-associated kinases (ibrutinib and idelalisib) and the antiapoptotic protein Bcl-2 (venetoclax) has dramatically changed treatments algorithms of CLL as well as the role of different adverse prognosticators. The marked benefit of these new drugs has been investigated in the context of NOTCH1 mutations (M). In fact, NOTCH1 M were significantly correlated with CD49d overexpression identifying CLL with reduced lymphocytosis and inferior nodal response (Tissino, 2018). Moreover, NOTCH1 M were characterized by overexpression and increased activity of the NF-kB pathway genes, promoting tumor cell proliferation and survival (Benedetti, 2017). The primary aims of our clinical research were: i) to correlate NOTCH1 M with CD49d expression and bax/bcl-2 ratio in ibrutinib-treated patients; ii) to verify the impact of NOTCH1M on the peripheral lymphocytes redistribution and on the nodal response calculated as percentual reduction from baseline (SPD); iii) to evaluate the impact of NOTCH1 M on overall response rate (ORR), progression free survival (PFS) and overall survival (OS); iiii) finally, to assess NOTCH1 M as an independent prognostic factor. Therefore, we evaluated the efficacy of ibrutinib as single agent, in a real-life contest, on 180 patients recruited from three independent cohorts from Italy, median age 69 years (36-90), median number of previous regimens 2 [range 0-4; 26 patients (14.4%) previously untreated]. Noteworthy, 24/64 (37.5%) TP53 mutated patients were treated in first line with ibrutinib (p<0.0001). Patients received 420 mg oral ibrutinib once daily until progression or occurrence of unacceptable side effects. Median follow up on TA was 25 months. NOTCH1 M were investigated with next generation sequencing (NGS) method. CD49d antigen was evaluated by flow cytometry and the threshold of positivity was set >30%. Bax/bcl-2 ratio, evaluated in 113 patients, was calculated by flow cytometry, dividing mean florescence intensity (MFI) of bax by MFI of bcl-2 on CLL cells. The threshold of positivity was set at the median value >1.5 (range 0.41-5.10). Sixty-five patients were NOTCH1 M (36.11%). NOTCH1 M were strongly correlated both with CD49d >30% (51/65; p=0.0001) and bax/bcl-2 ratio <1.5 (34/38; p=0.00007). Absolute lymphocyte counts (ALCs) were collected at days ranging from 30 to 90 on ibrutinib. NOTCH1 M were correlated with significant lower median ALCs than all other patients (10.7 x 106/ml vs 31.0 x 106/ml; p=0.0003). Moreover, the median SPD, calculated at 3-6 months on ibrutinib, was lower in NOTCH1 M patients (53% vs 80%; p<0.0001), confirming a significant poor nodal response. ORR was 90% [complete response (CR): 18%, partial response (PR): 28%, PR with lymphocytosis (PR-L): 44%]. The estimate 2-year PFS and OS were 80% and 84%, respectively. Sixty nine patients (39%) discontinued ibrutinib either for progression (n=38) or for adverse events (n=31). With regard to clinical outcome, NOTCH1 M were significantly correlated with PR and PR-L (30/65 and 22/65, respectively; p=0.00002). Moreover, NOTCH1M were significantly associated with disease recurrence (23/38; p=0.0005). Significant shorter PFS and OS were observed in NOTCH1 M patients (36% vs 84% and 58% vs 84% at 3 years, respectively; p<0.0001 and p=0.00075; Figure 1A and 1B). Thirty-seven patients underwent subsequently venetoclax [13 for toxicity (grade 3 or 4 WHO) and 24 for progression]. OS for this subgroup was 70% at 3 years (Figure 1C). In multivariate analysis of PFS, including previous chemotherapy regimens, NOTCH1, TP53 and IGHV status, NOTCH1 was confirmed as an independent prognostic factor (p=0.0002) together with TP53 (p=0.003). On the other hand, in multivariate analysis of OS, NOTCH1 remained as an independent prognostic factor (p=0.009) together with previous therapy (p=0.013) and TP53 (p=0.019). In conclusion, NOTCH1M are characterized by resistance to apoptosis, lower peripheral lymphocytosis and lower nodal shrinkage, all responsible for partial responses, subsequent relapses, shorter PFS and OS under ibrutinib treatment. The prognostic impact of NOTCH1 M on patients treated subsequently with venetoclax is unclear due to the low number of our cases (Roberts, 2019). Probably the therapeutic answer for NOTCH1 M patients could come either from TA combination approaches or from new gamma-secretase inhibitors or also from new antibodies targeting NOTCH1.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal