

Introduction
Relapses of diffuse large B-cell lymphoma typically occur within 2-3 years and only 10% of these patients reach a 3-year progression-free survival compared to 65% at diagnosis. Our ability to distinguish patients at risk for relapse remains based on clinical staging. We hypothesized that identifying genetic alterations in serial tumour biopsies at diagnosis and relapse would improve our ability to identify high-risk patients, make therapeutic selections and reveal molecular markers for chemo-immunotherapy resistant tumours. However, relatively few relapsed/refractory biopsies have been sequenced. A unique, clinically annotated, Nordic DLBCL cohort was used to identify significantly mutated genes, assess potential driver genes, comprehensively examine clonal evolution, and gauge the importance of clinical relapsed sampling.
Methods
To address the lack of information on the molecular foundations of relapsed/refractory DLBCL, we performed whole exome sequencing (WES) on 42 DLBCL cases, with 34% representing relapsed/refractory biopsies and 13 serially sample cases. Enriched with relapsed/refractory diffuse large B-cell lymphoma cases, we performed multiple computational analyses to identify significantly mutated genes (MutSig2CV), mutational signatures (NMF and DeConstructsSig), driver genes (IntOgen and CADD), clonal evolution architecture (SciClone and ClonEvol), druggable gene analysis (DGIdb), and HLA-inference and mutation calling (Polysolver).
Results
Clonal evolution analysis of 13 paired diagnostic and relapsed biopsies revealed that relapsed/refractory biopsies have remarkable similarities to diagnostic biopsies and often present with late divergent clonal evolution of the tumor. Mutational analysis of 18 serially sampled tumors determined that in the majority of cases druggable oncogenic variants do arise at relapse. In addition, time to relapse correlated with divergence of mutations from the diagnostic biopsy.
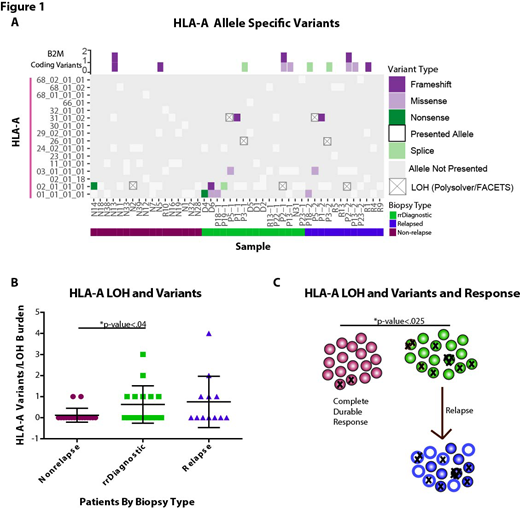
In addition to being identified as a significantly mutated gene, mutations in HLA-A had an increased incidence in cases that ultimately relapsed. This result led to an in-depth investigation into the mutational prevalence, timing, impact on prognosis, and loss of heterozygosity in the human leukocyte antigen (HLA) haplotypes of relapsed/refractory DLBCL. HLA-A mutagenesis and loss of heterozygosity was discovered as mechanisms of immune evasion in cases that go on to relapse from R-CHOP like therapies (Figure 1).
Conclusions
Our results yield insight into the development of chemo-immunotherapy resistant diffuse large B-cell lymphoma, and highlight the clinical importance of sampling relapsed biopsies. Analysis of immune evasion through MHC Class I/II, specifically HLA-A, may provide better characterization of patients for relapse prediction. In the age of personalized medicine it will be instrumental to determine if relapsed biopsies offer additional insight for salvage therapy treatment. Divergence of biopsies, as characterized by shared genomic mutations, increase with time and the majority of cases present with new alterations in druggable genes post-therapy.
Leppa:Roche: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Celgene: Consultancy; Bayer: Research Funding. Holte:Novartis: Honoraria, Other: Advisory board.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal