


Background
Systemic AL amyloidosis is a clonal plasma cell disorder in which amyloid fibrils are deposited in tissues and organs, leading to multi-system organ dysfunction. The most frequently involved organs are the heart and kidney (individually or together), with advanced cardiac involvement conferring particularly poor outcomes. Achievement of hematologic response and improved organ function result in better outcomes. There are currently no approved treatments for AL amyloidosis; multiple myeloma (MM) treatment strategies are used for these pts. Active, tolerable treatment options specific for AL amyloidosis are needed. The oral proteasome inhibitor (PI) ixazomib (ixa) is active and approved in combination with lenalidomide (L)-dexamethasone (Dex) for the treatment of MM pts who have received ≥1 prior therapy.
Methods
RRAL pts with measurable disease and major organ involvement (cardiac/renal) who required treatment after 1-2 prior therapies (and were not refractory to prior PI therapy) were randomized to ixa (4.0 mg, d 1, 8, 15) plus Dex (20 mg, d 1, 8, 15, 22) or physician's choice (Dex alone or plus melphalan [M], cyclophosphamide [C], thalidomide [T], or lenalidomide [L]) in 28-d cycles until disease progression or unacceptable toxicity (or best response plus 2 cycles or maximum 18 mos therapy/600 mg total dose for MDex). Randomization was stratified by cardiac risk stage, relapsed vs refractory disease, and prior PI exposure. Primary endpoints were 1) overall hematologic response rate (ORR) centrally adjudicated, and 2) death or vital organ deterioration at 2 yrs. Key secondary endpoints were overall survival (OS) and hematologic complete response (CR) rate; other secondary endpoints included hematologic/vital organ progression-free survival (PFS), time to vital organ deterioration or mortality, duration of hematologic response (DOR), and safety.
Results
168 pts were randomized to ixa-Dex (n=85) or physician's choice (n=83; 47 LDex, 24 MDex, 10 CDex, 2 TDex); median age was 65 (range 38-84) vs 66 (33-82) yrs, 60% vs 55% were male, 56% vs 63% had cardiac and 66% vs 58% had renal involvement (33% vs 23% had both) at initial diagnosis (plus 9% vs 12% liver, 12% vs 18% gastrointestinal tract, and 11% vs 10% peripheral nerve involvement), 47% vs 47% had prior bortezomib, and 47% vs 37% had prior transplant. Median time since diagnosis was 14.7 vs 15.9 mos.
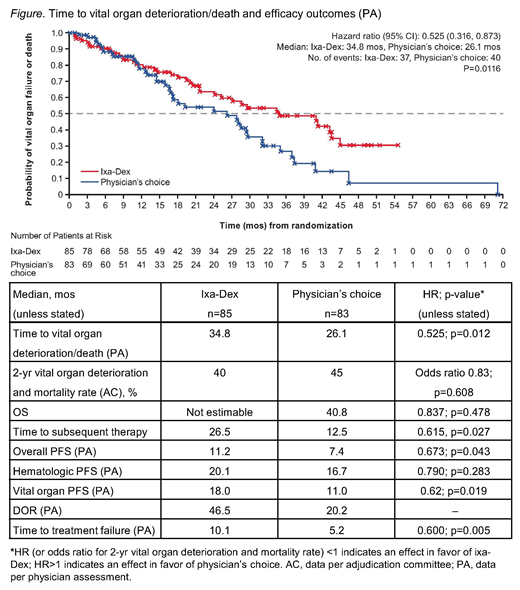
Hematologic responses were seen in 45 (53%) vs 42 (51%) pts receiving ixa-Dex vs physician's choice (odds ratio 1.10 [95% CI 0.60-2.01], p=0.762). Higher CR rates were seen with ixa-Dex vs physician's choice (26% vs 18%). Overall survival, overall/hematologic/vital organ PFS, time to vital organ deterioration/death, DOR, time to treatment failure, and time to subsequent therapy data all favored pts treated with ixa-Dex vs physician's choice (Figure). Vital organ response rates were 36% in the ixa-Dex arm vs 11% with physician's choice (cardiac response rate: 18% vs 5%; renal response rate: 28% vs 7%).
At data cut-off, pts had received a median treatment duration of 11.7 vs 4.9 mos with ixa-Dex vs physician's choice, and 21% vs 6% of pts remained on treatment. Grade ≥3 adverse events (AEs) were seen in 59% vs 56% of pts, including 33% vs 41% with drug-related grade ≥3 AEs, 45% vs 33% had serious AEs, 25% vs 20% had AEs resulting in discontinuation, and there were 6% vs 5% on-study deaths. AEs of clinical importance included diarrhea (34% vs 30%), rash (33% vs 20%), cardiac arrhythmias (25% vs 15%), nausea (24% vs 14%), pneumonia (22% vs 16%), and peripheral neuropathy (20% vs 15%). Common (≥5% overall) grade ≥3 AEs were fatigue (9% vs 9%), anemia (2% vs 10%), cardiac failure, dyspnea (each 6% vs 4%), peripheral edema, and pneumonia (each 5% vs 5%).
Conclusions
Treatment with ixa-Dex significantly prolonged duration of composite survival and vital organ function, PFS, and time to subsequent therapy vs physician's choice. Moreover, ixa-Dex resulted in an improved CR rate and DOR and, although the primary endpoint of hematologic response was not met, all clinically relevant time-to-event endpoint data favored ixa-Dex vs physician's choice. Ixa-Dex was generally well tolerated and associated with a doubling of treatment duration vs physician's choice; no new safety signals were seen. TOURMALINE-AL1 is the first phase 3 trial in RRAL to show significant outcome improvements, suggesting ixa-Dex represents a new option for RRAL pts, who have limited access to therapies.
Dispenzieri:Akcea: Consultancy; Intellia: Consultancy; Alnylam: Research Funding; Celgene: Research Funding; Takeda: Research Funding; Pfizer: Research Funding; Janssen: Consultancy. Kastritis:Amgen: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Takeda: Honoraria; Pfizer: Honoraria; Prothena: Honoraria; Genesis: Honoraria. Wechalekar:Takeda: Honoraria; GSK: Honoraria; Celgene: Honoraria; Amgen: Research Funding; Janssen-Cilag: Honoraria. Schönland:Prothena: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding; Medac: Other: Travel Grant. Sanchorawala:Proclara: Consultancy, Honoraria; Caelum: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Research Funding; Prothena: Research Funding; Celgene: Research Funding; Takeda: Research Funding. Landau:Pfizer: Membership on an entity's Board of Directors or advisory committees; Caelum: Membership on an entity's Board of Directors or advisory committees; Prothena: Membership on an entity's Board of Directors or advisory committees; Amgen: Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding; Karyopharm: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees. Suzuki:Takeda: Honoraria; BMS: Honoraria, Research Funding; Ono: Research Funding; Celgene: Honoraria; Janssen: Honoraria. Comenzo:Takeda: Research Funding; Caelum: Consultancy, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Karyopharm: Research Funding; Prothena Biosciences: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Sanofi-Aventis: Membership on an entity's Board of Directors or advisory committees; Unum: Membership on an entity's Board of Directors or advisory committees, Research Funding; Myself: Patents & Royalties: Patent 9593332, Pending 20170008966. Berg:Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Ltd: Employment, Patents & Royalties. Liu:Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited: Employment. Faller:Phoenicia Biosciences: Equity Ownership; Briacell Pharmaceuticals: Equity Ownership; Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited: Employment; Viracta Pharmaceuticals: Equity Ownership; Boston University: Employment.
Investigation of the oral proteasome inhibitor ixazomib in combination with dexamethasone versus physician's choice (of which there are no approved treatment options) for the treatment of relapsed/refractory primary systemic amyloidosis.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal