

Background: Immune Thrombocytopenia Purpura (ITP) can result in severely low platelet counts and while most of the 4,000 new cases of pediatric ITP diagnosed each year self-resolve, 10% of these patients have major bleeding episodes. The platelet count remains the mainstay method for predicting hemorrhage and unfortunately has only proven to be loosely correlated to bleeding severity. Consequently, there currently exists no biomarker that accurately and reliably predicts which patients need immediate medical treatment, all of which have side effects, and which patients only require monitoring. To that end, we leveraged our Platelet Contraction Cytometer (PCC), a versatile system that measures platelet contraction forces at the single-cell level and at high-throughput, to study platelets of patients with ITP prospectively. Buchanan bleeding scores were used to distinguish patients with severe symptoms from asymptomatic patients. With 49 patients, we observed two significant findings: 1) Tracking both single platelet force measurements and platelet count enables stratifying patients into having major, minor, or no risk for bleeding. Accordingly, patients in the major risk category have a combined low platelet force and low platelet count. 2) Longitudinal studies showed that when major risk patients had increased platelet force or higher platelet counts, this was associated with the alleviation of major symptoms. Thus, when utilized together, platelet force and platelet count can more accurately predict bleeding severity in pediatric ITP patients.
Platelet Contraction Cytometry: Our PCC utilizes a large array of fibrinogen "microdot" pairs patterned on a flat hydrogel of known stiffness. Thrombin-activated platelets adhere to these microdots, spread to the neighboring microdot, and contract, pulling the microdots closer together. As platelet force is directly proportional to the microdot displacement, only a single microscopy measurement is necessary to determine the force applied by each single platelet (Fig 1). As such, hundreds of platelets are measured in a controlled mechanical and biochemical environment (Myers et al, 2017)
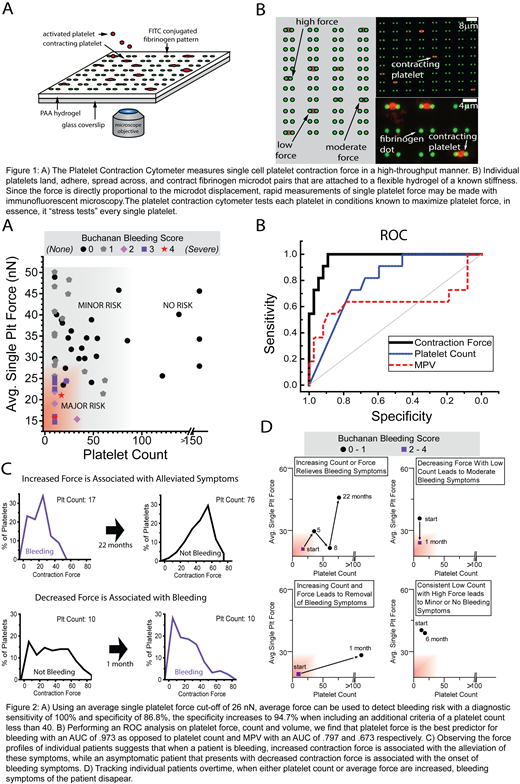
Results: With our cohort of 49 ITP patients, we observed that low average single cell platelet contraction forces highly correlate with severe bleeding symptoms (Buchannan scores 2-4). Using a regression tree, we found that an average force of 26nN best separates symptomatic from asymptomatic patients with a diagnostic sensitivity of 100% and specificity of 86.8% (AUC 0.97, 95% CI: 0.9361-1). However, platelets from some asymptomatic patients exerted forces of less than 26nN as well. In a more thorough examination, we found that majority of those asymptomatic patients with low platelet forces had platelet counts > 40,000/uL. Although our data shows that platelet count alone is a poor predictor of severe bleeding symptoms (AUC 0.8, 95% CI: 0.6757-0.9189), when a platelet count <40k/uL is coupled alongside our criterion of average contraction force <26 nN, we find that the specificity of our system increases to 94.7% and thus platelet count and platelet force synergistically predict which patients are symptomatic with high accuracy. Using a logistic regression model, we also found that with each 1nN decrease in average contraction force, the odds of the patient bleeding increases 2.1 (95% CI: 1.1-4.0) times that of being asymptomatic and when this decrease in contraction force is increased 5nN, the odds of a patient bleeding is 44.4 (95% CI: 1.8-1066.5) times that of being asymptomatic (Fig 2A-B).
Moreover, when tracking individual patients (n=4) over time, we demonstrate that whenever a patient's blood sample is associated with increased single platelet average contraction force >26 nN or platelet count >40k/uL, bleeding symptoms are alleviated. Conversely, whenever a patient exhibited high platelet contractile force and low platelet count, the onset of bleeding symptoms correlated with a decrease in platelet forces. Unlike bulk or micro-clot assays, our assay functions as a "stress test" of single platelets by placing them in conditions that maximize contractility, and in both cases, the reduction in the subpopulation of highly contractile platelets is correlated with bleeding severity. As such, our work suggests that single platelet forces could be used as a diagnostic biomarker to assess bleeding risk in patients with ITP regardless of count (Fig 2C-D).
Bennett:Novartis: Research Funding. Lam:Sanguina, LLC: Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal