

Introduction: Acquired thrombotic thrombocytopenic purpura (aTTP) is a rare, but life-threatening, hematological disorder characterized by severe thrombocytopenia, hemolytic microangiopathic anemia, and frequent organ damage. The underlying pathophysiology of aTTP is a functional deficiency of plasma ADAMTS13 activity caused by antibodies directed against the ADAMTS13 protease. Despite plasma exchange (PEX) and immunosuppression with corticosteroids, and, more recently, rituximab, which achieve remission in most patients with aTTP, 10-20% of patients are refractory to treatment and die as a result of disease progression. Most of such deaths occur during first episodes of aTTP, as subsequent relapses tend to be milder. These patients would probably benefit from new therapies aimed at temporarily halting the microvascular thrombosis. This study was aimed at identifying predictive factors of mortality during a first episode of aTTP.
Methods: We searched the Spanish TTP Registry (REPTT, Registro Español de la Purpura Trombocitopénica Trombótica) for patients with a clinical diagnosis of TTP (n = 345) with ADAMTS13 activity <10%, and anti-ADAMTS13 inhibitors in plasma (n = 143). Among these, we selected 103 patients with complete information on their first episode of aTTP. The patients were diagnosed between 2004 and 2018, and all were treated with daily PEX and corticosteroids. Additional treatments (rituximab, vincristine, etc.) were used at the discretion of the attending hematologist. Clinical and laboratory data of the episodes were analyzed at diagnosis and during the course of the treatment. The impact of refractoriness, exacerbations (as defined by the international consensus; DOI: 10.1111/jth.13571) and platelet transfusions on mortality was also studied.
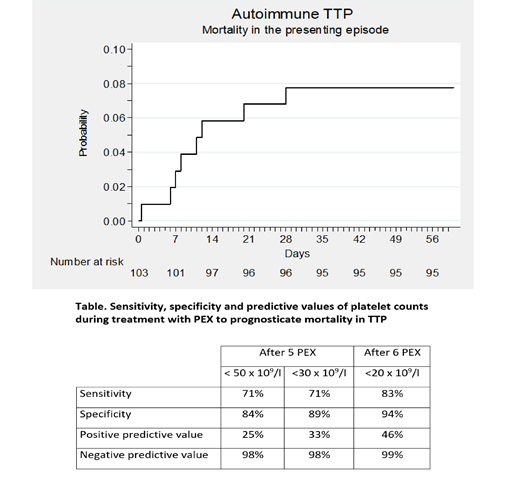
Results: The 103 patients examined suffered a total of 111 episodes of aTTP (103 with a first episode and 8 with a relapse). Eight deaths (7.7%) took place during an initial episode of aTTP and none during relapses. The time elapsed from the diagnosis to the events of death ranged from a few hours to 36 days (Figure). One patient died before starting the treatment. In the multivariate analysis, stupor or coma at diagnosis was the only clinical and biological factor associated with mortality, as 6 out of 18 patients with stupor or coma died vs. 2 out of 85 without these symptoms (OR: 21.95% CI: 4-114; p = 0.001).
Persistently low platelet counts during PEX (i.e. refractoriness) were also strong predictors of subsequent mortality, with a platelet count <20 x109/L after 6 PEX procedures yielding the highest positive and negative values (Table).
Exacerbation of aTTP while on treatment occurred in 44 of the 95 patients, all of whom eventually achieved remission with no events of death. Patients with exacerbations required a higher number of PEX procedures to achieve clinical remission (23, IQR: 19-31 vs. 12, IQR: 8-16; p <0.001) and were more likely to receive rituximab (39% vs. 9%; p = 0.001). Platelets were transfused into 16 patients, including 2 patients who died a few days later and 14 survivors.
Conclusions: Stupor or coma at diagnosis and lack of response to PEX by the 6th-7th day in patients experiencing first episodes of aTTP are strong predictors of mortality. These patients are candidates for new treatments aimed at controlling the microvascular thrombotic phenomena until effective immunosuppression is achieved. Disease exacerbation does not seem to increase mortality but requires a more intensive treatment.
De La Rubia:Celgene Corporation: Consultancy; AbbVie: Consultancy; AMGEN: Consultancy; Janssen: Consultancy; Takeda: Consultancy. Pascual Izquierdo:Novartis: Consultancy; Sanofi: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal