

Background: Deficiency of plasma ADAMTS13 activity resulting from acquired autoantibody against ADAMTS13 is the primary cause of immune thrombotic thrombocytopenic purpura (iTTP). Therapeutic plasma exchange plus corticosteroids and immunosuppression is the standard of care for patients with iTTP. However, mortality rate remains high and clinical factors or laboratory biomarkers that predict mortality are not fully established. Previous studies have demonstrated that plasma levels of histone-DNA complexes and cell-free DNA are dramatically elevated in patients with acute disease but reduced during remission. We hypothesize that elevated histone-DNA complexes or cell-free DNA may have a predictive role for mortality in patients with acute iTTP.
Methods: 102 unique patients with a confirmed diagnosis of iTTP who underwent therapeutic plasma exchange (TPE) at UAB-Medical Center from April 2006 to December 2018 were enrolled into the study. Demographic information and laboratory parameters were collected on admission and during the follow-up. Plasma levels of histone-DNA complexes and cell-free DNA were determined by an enzyme-linked immunosorbent assay and PicoGreen dsDNA assay, respectively. Mann-Whitney, Fisher's exact, t test, log-rank test, and Cox proportional hazard regression analysis were performed to determine the significance of each marker in predicting death.
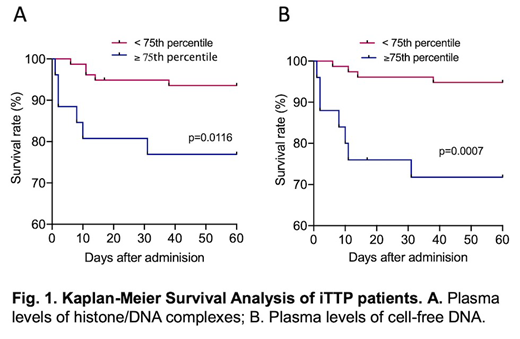
Results: In this cohort, age was 44.7 ± 1.3 (mean ± SD) years old, 56.9% were female, 82.4% were African Americans, 61.8% had an initial episode, the median (IQR) body mass index (BMI) was 33.6 (29.3-41.5). 52.9% of patients had hypertension, 21.6% diabetes, 18.6% systemic lupus erythematous and 8.7% HIV. The overall mortality rate was 10.8% (11/102). Plasma levels, median (IQR), of histone-DNA complexes and cell-free DNA on admission were 56.3 (35.8-136.4) AU/mL and 952.2 (799.7-1431.4) ng/mL, respectively. Mann-Whitney test revealed that high plasma levels of histone-DNA complex (≥134.9 U/mL) (p=0.007) and cell-free DNA (≥952.2 ng/mL) (p=0.009) were associated with the increased risks of myocardial injury (e.g. elevated troponin). Cox proportional hazard regression analysis demonstrated that the increased levels of histone-DNA complexes and cell-free DNA were also predictive for the increased mortality rates in patients with iTTP with hazard ratios (HRs) of 4.1 (95% CI, 1.2-13.4) (p=0.02) and 8.5 (95% CI, 2.2-33.3 (p=0.002), respectively. Kaplan-Meier survival analysis revealed significant differences in the disease-free survival rates of patients with high levels (≥75 percentile) vs. low levels (<75 percentile) of plasma histone-DNA complexes and cell-free DNA, respectively (see Fig. 1).
Conclusion: Our results demonstrate that the elevated plasma levels of histone-DNA complexes and cell-free DNA predict the worse outcome (e.g. the increased mortality rates) in patients with iTTP.
*SD, standard deviation; IQR, interquartile range; 95% CI, 95% confidential interval.
Zheng:Ablynx/Sanofi: Consultancy, Speakers Bureau; Alexion: Speakers Bureau; Shire/Takeda: Research Funding; Clotsolution: Other: Co-Founder.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal