

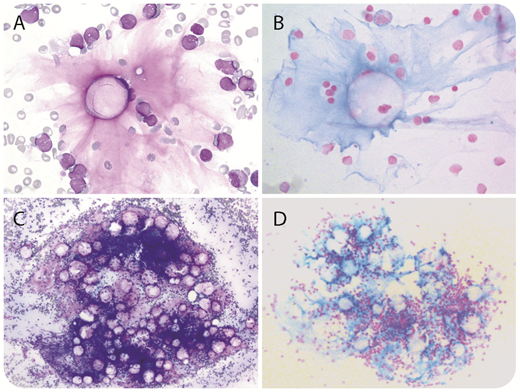
A 13-year-old boy was referred for weight loss, polyuria, polydipsia, asthenia, and pancytopenia. Bone marrow (BM) smears revealed the presence of 81% medium-sized lymphoblasts. A diagnosis of B-cell acute leukemia (European Group for the Immunological Characterization of Leukemias stage B-II) with t(12;21) ETV6-RUNX1 rearrangement was established. Unexpectedly, BM smear examination also revealed amorphous bluish-pink substance deposits within the stroma associated with microadipocytes (panels A and C; May-Grünwald-Giemsa stain, 60× and 10× objectives, respectively). Alcian blue staining confirmed the gelatinous transformation of the BM (GTBM; panels B and D; 60× and 10× objectives, respectively). No BM biopsy was performed. Simultaneously, blood tests displayed marked hyperglycemia combined with elevated glycated hemoglobin. Increases of anti-insulin, anti-GAD, and anti–IA-2A autoantibody levels further demonstrated the concomitance of GTBM, type-1 diabetes mellitus, and lymphoblastic leukemia.
GTBM features include adipocyte atrophy, hematopoietic tissue hypoplasia, and extracellular deposition of gelatinous substance (acid mucopolysaccharides). GTBM has been described in association with various chronic malnutrition conditions and is usually seen in anorexia nervosa, AIDS, or cachexia. In rare cases, GTBM has been reported at diagnosis of acute leukemia, but it has also been described in other abnormal metabolic conditions, such as diabetes mellitus, as described here. No GTBM was observed after induction chemotherapy and diabetes mellitus management. The patient remains in remission after consolidation with undetectable ETV6-RUNX1 transcript but subnormal complete blood count.
A 13-year-old boy was referred for weight loss, polyuria, polydipsia, asthenia, and pancytopenia. Bone marrow (BM) smears revealed the presence of 81% medium-sized lymphoblasts. A diagnosis of B-cell acute leukemia (European Group for the Immunological Characterization of Leukemias stage B-II) with t(12;21) ETV6-RUNX1 rearrangement was established. Unexpectedly, BM smear examination also revealed amorphous bluish-pink substance deposits within the stroma associated with microadipocytes (panels A and C; May-Grünwald-Giemsa stain, 60× and 10× objectives, respectively). Alcian blue staining confirmed the gelatinous transformation of the BM (GTBM; panels B and D; 60× and 10× objectives, respectively). No BM biopsy was performed. Simultaneously, blood tests displayed marked hyperglycemia combined with elevated glycated hemoglobin. Increases of anti-insulin, anti-GAD, and anti–IA-2A autoantibody levels further demonstrated the concomitance of GTBM, type-1 diabetes mellitus, and lymphoblastic leukemia.
GTBM features include adipocyte atrophy, hematopoietic tissue hypoplasia, and extracellular deposition of gelatinous substance (acid mucopolysaccharides). GTBM has been described in association with various chronic malnutrition conditions and is usually seen in anorexia nervosa, AIDS, or cachexia. In rare cases, GTBM has been reported at diagnosis of acute leukemia, but it has also been described in other abnormal metabolic conditions, such as diabetes mellitus, as described here. No GTBM was observed after induction chemotherapy and diabetes mellitus management. The patient remains in remission after consolidation with undetectable ETV6-RUNX1 transcript but subnormal complete blood count.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal