

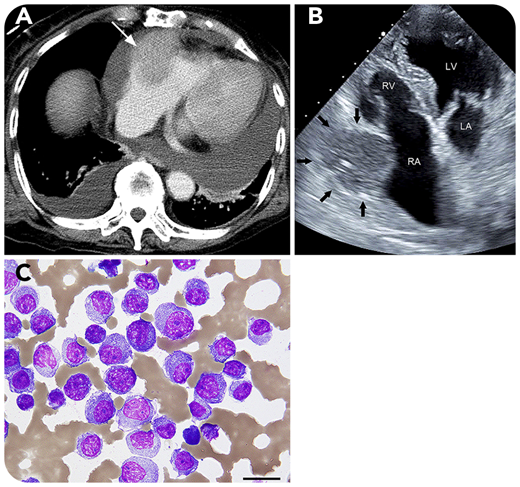
A 79-year-old woman visited our hospital because of back pain. Laboratory examination showed monoclonal λ light chains in the serum, and a population of 60% CD138+ plasma cells was found on bone marrow biopsy. Karyotype was normal, and whole-body computed tomography (CT) found no extramedullary lesions. She was diagnosed with immunoglobulin A λ-type multiple myeloma (MM), classified as stage 2 according to the Revised International Staging System; she started treatment with bortezomib plus dexamethasone and achieved complete response. One year later, multiple tumors in her right mammary gland were detected on CT. Mammary gland biopsy found plasmacytoma, resulting in a diagnosis of extramedullary lesions in MM. Four years after first visit, she was admitted with heart failure. Contrast-enhanced CT (panel A) and echocardiography (panel B; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle) revealed a moderate amount of pericardial effusion and a mass (3.8 × 4.5 cm) in the right atrial wall (white arrow in panel A and black arrows in panel B) consistent with cardiac tamponade; pericardial drainage was then performed. Cytology for the bloody pericardial effusion showed clusters of plasma cells (panel C; periodic acid Schiff stain; original magnification ×400), indicating an extramedullary lesion to the pericardium. Fluorescence in situ hybridization from the bone marrow detected no cytogenetic abnormality. Although daratumumab, carfilzomib, and pomalidomide were administered, the mass enlarged, and she died thereafter.
Extramedullary lesions of MM mostly occur near the axial skeleton by direct infiltration from the bone marrow. However, cardiac lesions are rare.
A 79-year-old woman visited our hospital because of back pain. Laboratory examination showed monoclonal λ light chains in the serum, and a population of 60% CD138+ plasma cells was found on bone marrow biopsy. Karyotype was normal, and whole-body computed tomography (CT) found no extramedullary lesions. She was diagnosed with immunoglobulin A λ-type multiple myeloma (MM), classified as stage 2 according to the Revised International Staging System; she started treatment with bortezomib plus dexamethasone and achieved complete response. One year later, multiple tumors in her right mammary gland were detected on CT. Mammary gland biopsy found plasmacytoma, resulting in a diagnosis of extramedullary lesions in MM. Four years after first visit, she was admitted with heart failure. Contrast-enhanced CT (panel A) and echocardiography (panel B; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle) revealed a moderate amount of pericardial effusion and a mass (3.8 × 4.5 cm) in the right atrial wall (white arrow in panel A and black arrows in panel B) consistent with cardiac tamponade; pericardial drainage was then performed. Cytology for the bloody pericardial effusion showed clusters of plasma cells (panel C; periodic acid Schiff stain; original magnification ×400), indicating an extramedullary lesion to the pericardium. Fluorescence in situ hybridization from the bone marrow detected no cytogenetic abnormality. Although daratumumab, carfilzomib, and pomalidomide were administered, the mass enlarged, and she died thereafter.
Extramedullary lesions of MM mostly occur near the axial skeleton by direct infiltration from the bone marrow. However, cardiac lesions are rare.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal