

Key Points
Pembrolizumab provided durable and deep responses with acceptable tolerability in a broad spectrum of RRcHL.
Pembrolizumab was also effective in difficult-to-treat chemorefractory cHL.

Abstract
Programmed death-1 inhibitors are approved for patients with relapsed or refractory classic Hodgkin lymphoma (RRcHL). We present the 2-year follow-up of the phase 2 KEYNOTE-087 study of pembrolizumab in 210 patients, based on HL progression after autologous stem cell transplantation (ASCT) and subsequent brentuximab vedotin (BV; cohort 1); salvage chemotherapy and BV, with ineligibility for SCT owing to chemorefractory disease (cohort 2); and progression after SCT without BV (cohort 3). With a median follow-up of 27.6 months, the objective response rate (ORR) by blinded independent central review was 71.9% (95% CI, 65.3-77.9), the complete response rate (CRR) was 27.6%, and the partial response (PR) rate was 44.3%. Median duration of response was 16.5 months (range, 0.0+ to 27.0+ [+, no progressive disease at last assessment]) in all patients, 22.1 months in cohort 1, 11.1 months in cohort 2, and 24.4 months in cohort 3. Median progression-free survival was not reached in all patients with CR: 13.8 months (95% CI, 12.0-22.1) for patients with PR and 10.9 months (95% CI, 5.6-11.1) for patients with stable disease. Median overall survival was not reached in all patients or in any cohort. Treatment-related adverse events (TRAEs) of any grade occurred in 153 (72.9%) patients; grades 3 and 4 occurred in 25 (12.0%) patients; none resulted in death. Results confirmed effective antitumor activity, durability of response, and manageable safety of pembrolizumab monotherapy in RRcHL, regardless of prior treatment and including chemoresistant cHL. This trial was registered at www.clinicaltrials.gov as #NCT02453594.
Introduction
The inhibitors of programmed death 1 (PD-1)—nivolumab and pembrolizumab—showed effective antitumor activity and tolerable safety in patients with classic Hodgkin lymphoma (cHL) that progressed after autologous stem cell transplantation (ASCT) and/or brentuximab vedotin (BV).1,,-4 PD-1 inhibitors can be considered for the treatment of patients with refractory cHL who are ineligible for ASCT because of comorbidity or failure of first salvage chemotherapy or relapsed disease after ASCT, with or without BV.5 Both drugs were approved with limited follow-up by the US Food and Drug Administration based on phase 1 and 2 studies.6,7 Pertinent outstanding questions are the durability of response with PD-1 inhibitors and whether durable remission can be achieved in patients with a broad spectrum of relapsed or refractory cHL (RRcHL).
Previously, we reported the safety and efficacy of pembrolizumab in patients with RRcHL from the phase 2 KEYNOTE-087 study.4 With a median follow-up of 10.1 months, pembrolizumab showed excellent antitumor activity, with an overall response rate (ORR) of 69.0% and a complete response (CR) rate of 22.4% in all patients; 75.6% of patients had responses lasting at least 6 months. Here, we present results with an additional follow-up of ∼17.5 months, to evaluate the durability of response to pembrolizumab. We also present exploratory efficacy analyses in patient subgroups by prior treatment, such as BV naive, BV before ASCT, and BV after ASCT. Last, we present efficacy and safety data of a second course of pembrolizumab. Results of a second course may lead to the use of pembrolizumab as an additional treatment option for patients whose disease progresses after CR with pembrolizumab.
Patients and methods
KEYNOTE-087 was a multicenter, single-arm, multicohort, nonrandomized phase 2 study of pembrolizumab in patients with RRcHL. Patients were enrolled in 3 cohorts based on cHL progression after ASCT and subsequent BV (cohort 1); salvage chemotherapy and BV, with ineligibility for ASCT owing to chemorefractory disease (cohort 2); and progression after ASCT without subsequent BV (cohort 3). In cohort 2, chemorefractory was defined as failure to achieve CR or partial response (PR) to salvage therapy. Cohort 3 included BV-naive and BV-treated patients; some had received BV as part of primary treatment or salvage therapy. Detailed methods have been published.4
Eligible patients were aged ≥18 years, had measurable disease (Eastern Cooperative Oncology Group performance status of 0 or 1) and adequate organ function and were able to provide a new or archival evaluable core or excisional lymph node biopsy sample at screening for biomarker analysis. All patients provided written informed consent before study entry. The protocol and all amendments were approved by the independent institutional review board or ethics committees for each site. The study was conducted in accordance with the guidelines of the International Conference on Harmonization Guidelines for Good Clinical Practice and the Declaration of Helsinki.
Study design and treatment
Patients were treated with pembrolizumab 200 mg intravenously every 3 weeks for up to 2 years or until documented confirmed disease progression, occurrence of intolerable toxicity, or patient or investigator decision to withdraw from the study. Based on investigator decision, patients achieving CR could stop pembrolizumab after receiving a minimum of 24 weeks of treatment if at least 2 doses of pembrolizumab were received after confirmation of CR per 2007 International Working Group Revised Response Criteria for Malignant Lymphomas (RRC).8 Patients who met this criterion were permitted to receive additional pembrolizumab treatment of up to 12 months upon relapse, if the patient had not received any anticancer treatment since the last dose of pembrolizumab and continued to meet eligibility criteria for study.
Assessments
Response was assessed by computed tomography every 12 weeks per RRC.8 Positron emission tomography was performed at weeks 12 and 24, to confirm CR or progressive disease (PD), and as clinically indicated. Primary end points were safety and overall response rate (ORR), defined as the proportion of patients who had response (CR or PR), by blinded independent central review (BICR) per RRC8 in all patients and in the 3 cohorts. Secondary end points were CR rate by BICR, progression-free survival (PFS) and duration of response (DOR) by BICR per RRC, and overall survival (OS). Exploratory objectives included ORR, complete response rate (CRR), PFS, DOR, and OS for patients in subgroups based on prior BV use: BV naive, BV before ASCT, and BV after ASCT. Additional exploratory analyses involved ORR, CRR, PR rate (assessed by investigator review), and DOR by investigator review in patients treated with a second pembrolizumab course.
Patients were monitored for adverse events (AEs), serious AEs, and immune-mediated AEs. AEs were graded per National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0. Immune-mediated AEs were based on a list of terms specified by the sponsor and included by the investigator regardless of attribution to study treatment or immune relatedness.
Statistical analysis
Efficacy and safety were analyzed in the all-subjects-as-treated population of all patients who received at least 1 dose of study drug. ORR and CR were assessed for the overall population and by each cohort. The ORR assessment involved the point estimate and 95% 2-sided binomial exact confidence interval using the Clopper-Pearson method. PFS, OS, and DOR were estimated using the Kaplan-Meier method.
Results
Patients and disposition
At data cutoff (21 March 2018), of the 210 patients enrolled and treated in the 3 cohorts, 39 (18.6%) had completed treatment, and 5 (2.4%) were still receiving treatment. Of the 166 (79.0%) patients who discontinued treatment, the most common cause of discontinuation across all cohorts was disease progression (n = 86, 41.0%), followed by CR (n = 28, 13.3%) and AEs (n = 18, 8.6%; supplemental Figure 1, available on the Blood Web site). Median age was 35 years (range, 18-76). Patients had received a median of 4 prior lines of therapy (range, 1-12; supplemental Table 1). All patients in cohorts 1 and 2 had received prior BV, per study design, and 25 (41.7%) patients in cohort 3 had received prior BV.4 Median follow-up was 27.6 months (range, 1.0-32.9). Patients received a median of 21, 12, and 19.5 doses in their first course of pembrolizumab in cohorts 1, 2, and 3, respectively.
Objective responses in all patients
ORR by BICR in all patients was 71.9% (95% CI, 65.3-77.9) with a CRR of 27.6% and PR rate of 44.3% (Table 1). ORR was 76.8% in cohort 1, 66.7% in cohort 2, and 73.3% in cohort 3 (Table 1). Among patients who achieved CR (n = 58), 84.5% did so after ≥6 months of treatment and 63.8% did so after ≥12 months of treatment. Median time to response (TTR) was 2.8 months (range, 2.1-16.5) in all patients and was similar in patients in each cohort (supplemental Table 2). Median DOR was 16.5 months (range, 0.0+ to 27.0+ months [+, no progressive disease at last assessment]) in all responders (Figure 1A; supplemental Table 2). Median DOR was 22.1 months in cohort 1, 11.1 months in cohort 2, and 24.4 months in cohort 3 (Figure 1A; supplemental Table 2). Of 151 responders, 37 (24.5%) had ongoing responses. By Kaplan-Meier estimates, 61 (58.5%) had responses lasting ≥12 months, and 16 (42.5%) had responses lasting ≥24 months (Figure 1A). Sixteen (30.2%) patients in cohort 1, 8 (14.8%) in cohort 2, and 13 (29.5%) in cohort 3 had ongoing responses.
Best overall response by blinded independent central review
| Cohort 1 (n = 69): after ASCT/BV | Cohort 2 (n = 81): ineligible for ASCT and treatment failure with BV therapy | Cohort 3 (n = 60): no BV after ASCT | All patients (N = 210) | |||||
|---|---|---|---|---|---|---|---|---|
| n (%) | 95% CI* | n (%) | 95% CI* | n (%) | 95% CI* | n (%) | 95% CI* | |
| ORR | 53 (76.8) | 65.1-86.1 | 54 (66.7) | 55.3-76.8 | 44 (73.3) | 60.3-83.9 | 151 (71.9) | 65.3-77.9 |
| CR† | 18 (26.1) | 16.3-38.1 | 21 (25.9) | 16.8-36.9 | 19 (31.7) | 20.3-45.0 | 58 (27.6) | 21.7-34.2 |
| PR | 35 (50.7) | 38.4-63.0 | 33 (40.7) | 29.9-52.2 | 25 (41.7) | 29.1-55.1 | 93 (44.3) | 37.5-51.3 |
| SD | 9 (13.0) | 6.1-23.3 | 7 (8.6) | 3.5-17.0 | 7 (11.7) | 4.8-22.6 | 23 (11.0) | 7.1-16.0 |
| PD | 5 (7.2) | 2.4-16.1 | 18 (22.2) | 13.7-32.8 | 9 (15.0) | 7.1-26.6 | 32 (15.2) | 10.7-20.8 |
| No assessment | 2 (2.9) | 0.4-10.1 | 2 (2.5) | 0.3-8.6 | 0 (0) | — | 4 (1.9) | 0.5-4.8 |
| Cohort 1 (n = 69): after ASCT/BV | Cohort 2 (n = 81): ineligible for ASCT and treatment failure with BV therapy | Cohort 3 (n = 60): no BV after ASCT | All patients (N = 210) | |||||
|---|---|---|---|---|---|---|---|---|
| n (%) | 95% CI* | n (%) | 95% CI* | n (%) | 95% CI* | n (%) | 95% CI* | |
| ORR | 53 (76.8) | 65.1-86.1 | 54 (66.7) | 55.3-76.8 | 44 (73.3) | 60.3-83.9 | 151 (71.9) | 65.3-77.9 |
| CR† | 18 (26.1) | 16.3-38.1 | 21 (25.9) | 16.8-36.9 | 19 (31.7) | 20.3-45.0 | 58 (27.6) | 21.7-34.2 |
| PR | 35 (50.7) | 38.4-63.0 | 33 (40.7) | 29.9-52.2 | 25 (41.7) | 29.1-55.1 | 93 (44.3) | 37.5-51.3 |
| SD | 9 (13.0) | 6.1-23.3 | 7 (8.6) | 3.5-17.0 | 7 (11.7) | 4.8-22.6 | 23 (11.0) | 7.1-16.0 |
| PD | 5 (7.2) | 2.4-16.1 | 18 (22.2) | 13.7-32.8 | 9 (15.0) | 7.1-26.6 | 32 (15.2) | 10.7-20.8 |
| No assessment | 2 (2.9) | 0.4-10.1 | 2 (2.5) | 0.3-8.6 | 0 (0) | — | 4 (1.9) | 0.5-4.8 |
Based on binomial exact CI method.
For complete remission, a residual mass was permitted for patients who had negative results, as seen on positron emission tomography.
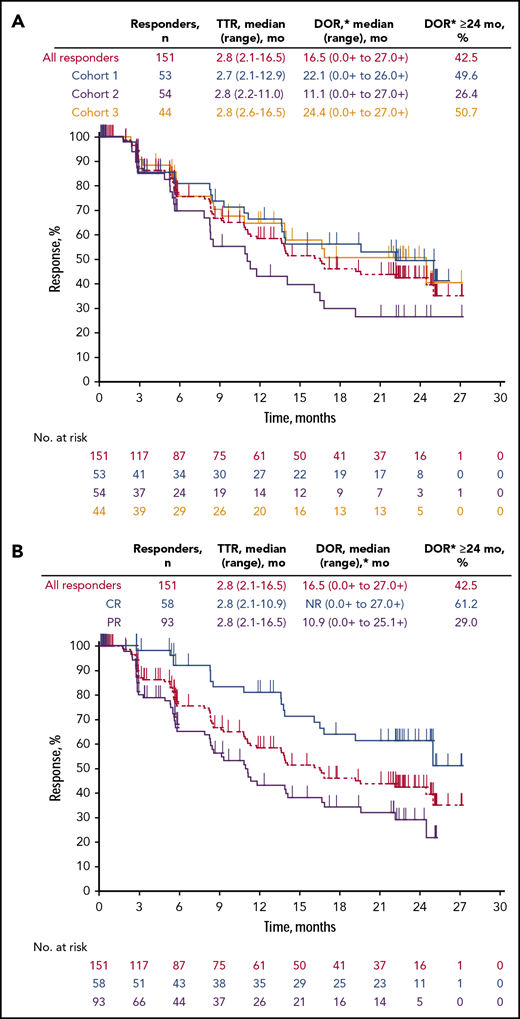
Kaplan-Meier estimate of duration of response. Responders by cohort (A) and by best response (B). *Based on Kaplan-Meier estimate.
Kaplan-Meier estimate of duration of response. Responders by cohort (A) and by best response (B). *Based on Kaplan-Meier estimate.
Of the 58 patients who achieved CR, median TTR was 2.8 months (range, 2.1-10.9). For all patients with CR, median DOR was not reached (Figure 1B) and was 25.0 months in cohort 1, 19.2 months in cohort 2, and not reached in cohort 3 (supplemental Table 2).
Of the 93 patients who achieved PR, TTR was 2.8 months. Median DOR was 10.9 months in all patients who had PR (Figure 1B; supplemental Table 2), 19.5 months in cohort 1, 7.9 months in cohort 2, and 13.9 months in cohort 3.
PFS in all patients
Median PFS was 13.7 months (95% CI, 11.1-17.0) in all patients, 16.4 months in cohort 1, 11.1 months in cohort 2, and 19.4 months in cohort 3 (Figure 2A). Median PFS was not reached in patients with CR (Figure 2B, supplemental Table 3) and was 13.8 months in all patients with PR (supplemental Table 3). Median PFS in patients with PR by cohort was 22.2 months in cohort 1 (Figure 2C), 13.4 months in cohort 2 (Figure 2D), and 19.4 months in cohort 3 (Figure 2E). In the 23 patients who had stable disease (SD), median PFS was 10.9 months (95% CI, 5.6-11.1) in the total patient population, 10.9 months (95% CI, 5.4-11.0) in cohort 1, 13.3 months (95% CI, 5.3 to not reached [NR]) in cohort 2, and 10.3 months (95% CI, 5.6-19.9) in cohort 3.
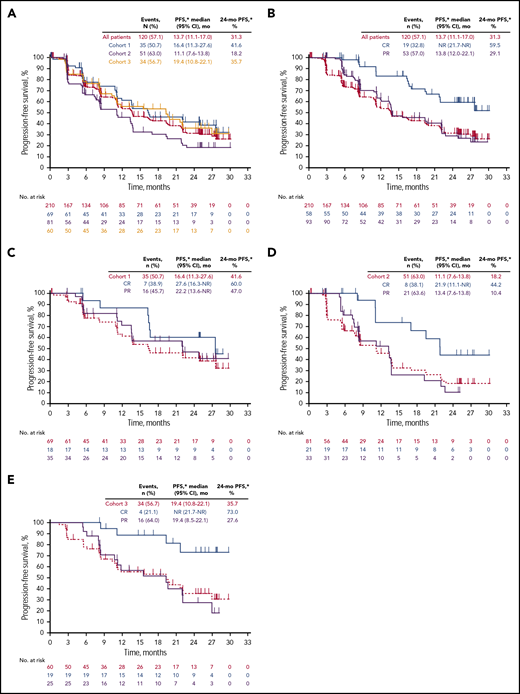
Kaplan-Meier estimate of PFS. In all patients and by cohort (A) and patients with complete or PR in all patients (B), cohort 1 (C), cohort 2 (D), and cohort 3 (E). *Based on Kaplan-Meier method for censored data.
Kaplan-Meier estimate of PFS. In all patients and by cohort (A) and patients with complete or PR in all patients (B), cohort 1 (C), cohort 2 (D), and cohort 3 (E). *Based on Kaplan-Meier method for censored data.
OS in all patients
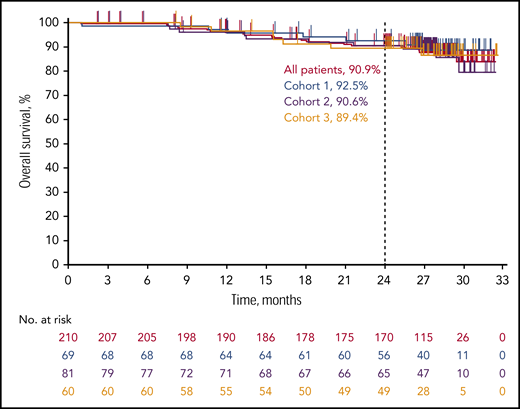
Median OS was not reached in all patients or in any cohort (Figure 3). The 24-month OS rate in patients with CR was 100.0% in all 3 cohorts. Among patients who achieved PR, the 24-month OS rates were 91.1% in all patients, 94.3% for patients in cohort 1, 90.4% in cohort 2, and 87.7% in cohort 3. The 24-month OS rates were 84.2% in all patients who had SD, 85.7% in cohort 1, and 83.3% in cohorts 2 and 3. Among patients who experienced PD, the 24-month OS rate was 60.0% in cohort 1, 82.4% in cohort 2, and 77.8% in cohort 3.
Efficacy outcomes in subgroups by prior treatment
In subgroups by BV use, ORR was 77.1% in BV-naive patients (n = 35), 70.6% in patients who received BV before ASCT (n = 17), and 80.0% in patients who received BV after ASCT (n = 25; supplemental Table 4). Median TTR was 2.8 months in BV-naive patients, 4.2 months in patients who received BV before ASCT, and 2.7 months in patients who received BV after ASCT (supplemental Table 4). Median DOR was 24.4 months in BV-naive patients, 13.9 months in patients receiving BV before ASCT, and not reached in patients who received BV after ASCT. Median PFS was 19.4 months (95% CI, 8.1-NR) in BV-naive patients, 19.7 (95% CI, 5.5-22.1) in patients who received BV before ASCT, and 24.9 months (95% CI, 10.9-NR) in patients who received BV after ASCT. Median OS was not reached in BV-naive patients; the 24-month OS rate was 91.2%. The 24-month OS rate was 86.2% in patients who received BV before ASCT and 96.0% in patients who received BV after ASCT.
Response characteristics of patients treated with a second course of pembrolizumab
Ten patients (6 in cohort 1, 3 in cohort 2, and 1 in cohort 3) were treated with a second course of pembrolizumab (Table 2). Eight of 10 patients were evaluable for response (had reached the week 12 second-course assessment or discontinued before it). The ORR, per investigator review, was 75% (6 of 8). Of the 6 patients in cohort 1, 1 had CR with a response duration of 11.3 months and completed a second course of pembrolizumab treatment. Two patients had PR: 1 had a response duration of 5.6 months and was still on treatment at database cutoff, and the other had a response duration of 6.9 months and discontinued treatment because of disease progression (Figure 4). All 3 patients in cohort 2 had CR, 1 had a response duration of 8.3 months and was still on treatment, 1 had a response duration of 0.7 months and discontinued treatment because of an AE, and 1 completed a second course of treatment, with a response duration of 11.2 months. The cohort 3 patient had SD with a duration of 11.0 months.
Response characteristics and immune-mediated AEs and infusion reactions in patients treated with second pembrolizumab course
| Cohort/patient no.* | DOR, 1st course | BOR, 2nd course† | DOR, 2nd course | Response on 2nd course | Reason for 2nd course discontinuation | Immune-mediated AEs and infusion reactions‡ | |
|---|---|---|---|---|---|---|---|
| 1st course | 2nd course | ||||||
| Cohort 1 | |||||||
| 1 | 23.5 | NA§ | — | — | — | Uveitis | — |
| 3 | 14.5 | PR | 5.6 | Ongoing | — | — | — |
| 4 | 18.0 | NA§ | — | — | — | — | — |
| 6 | 10.8 | PR | 6.9 | — | Clinical progression | — | — |
| 8 | 8.3 | CR | 11.3 | Ongoing | Completed | Infusion reactions | — |
| 7¶ | 11.0 | PD | 5.3 | — | PD | — | — |
| Cohort 2 | |||||||
| 2 | 5.0 | CR | 8.3 | Ongoing | — | Sarcoidosis | Sarcoidosis |
| 10 | 8.3 | CR | 0.7 | — | AE | Pancreatitis | — |
| 9 | 5.3 | CR | 11.2 | Ongoing | Completed | Colitis | — |
| Cohort 3 | |||||||
| 5 | 7.1 | SD | 11.0 | — | Completed | — | — |
| Cohort/patient no.* | DOR, 1st course | BOR, 2nd course† | DOR, 2nd course | Response on 2nd course | Reason for 2nd course discontinuation | Immune-mediated AEs and infusion reactions‡ | |
|---|---|---|---|---|---|---|---|
| 1st course | 2nd course | ||||||
| Cohort 1 | |||||||
| 1 | 23.5 | NA§ | — | — | — | Uveitis | — |
| 3 | 14.5 | PR | 5.6 | Ongoing | — | — | — |
| 4 | 18.0 | NA§ | — | — | — | — | — |
| 6 | 10.8 | PR | 6.9 | — | Clinical progression | — | — |
| 8 | 8.3 | CR | 11.3 | Ongoing | Completed | Infusion reactions | — |
| 7¶ | 11.0 | PD | 5.3 | — | PD | — | — |
| Cohort 2 | |||||||
| 2 | 5.0 | CR | 8.3 | Ongoing | — | Sarcoidosis | Sarcoidosis |
| 10 | 8.3 | CR | 0.7 | — | AE | Pancreatitis | — |
| 9 | 5.3 | CR | 11.2 | Ongoing | Completed | Colitis | — |
| Cohort 3 | |||||||
| 5 | 7.1 | SD | 11.0 | — | Completed | — | — |
BOR, best overall response; NA, not applicable.
Per duration of response graph (Figure 4).
By site review per International Working Group Revised Response Criteria for Malignant Lymphoma.
Based on a list of terms specified by the sponsor and included by the investigator, regardless of attribution to study treatment or immune relatedness; related terms are included.
At data cutoff, 2 patients had recently started a second course of pembrolizumab, and response assessment had not yet occurred.
Patient had an AE of pericarditis during the first course of pembrolizumab treatment that also occurred during the second course of treatment and was considered by the investigator to be immune-related.
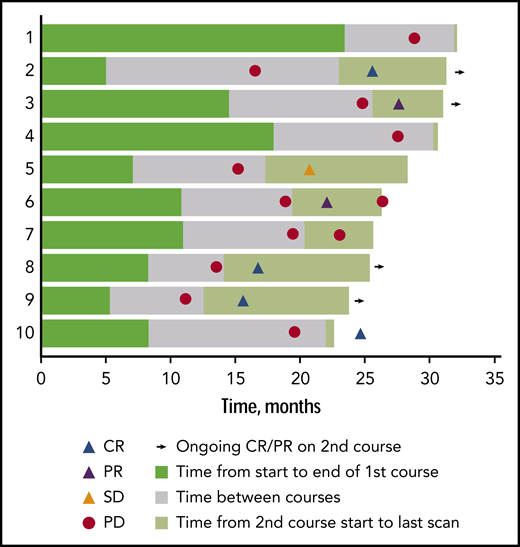
Duration of response in first course and second course in patients treated with a second pembrolizumab course. Patient 10 discontinued the second course because of an adverse event.
Duration of response in first course and second course in patients treated with a second pembrolizumab course. Patient 10 discontinued the second course because of an adverse event.
Safety
Treatment-related AEs occurred in 153 (72.9%) patients; most were mild to moderate: 60.9% had grades 1 and 2, and 11.0% had grade 3 treatment-related AEs (Table 3). None led to death. The most common grade 3 treatment-related AEs were neutropenia and diarrhea. Two patients had grade 4 treatment-related AEs (increased lipase and myocarditis, 1 each). Immune-mediated AEs were reported for 33.8% of patients: most were low grade (grades 3-5, 2.9%; Table 3). The most commonly reported immune-mediated AEs were hypothyroidism (15.7%), pneumonitis (4.8%), and hyperthyroidism (3.8%). Infusion-related reactions were reported in 5.2% of patients. Median time to onset of the first immune-related AE was 85 days (range, 1-787 days). Most immune-related AEs resolved without sequelae (67.6%); 21.1% of events were not resolved. The immune-mediated AE sarcoidosis occurred in the second course in 1 patient; this patient experienced the AE during the first course as well (Table 2). One patient had an AE of pericarditis during the first course of pembrolizumab treatment that also occurred during the second course of pembrolizumab treatment and was considered by the investigator to be immune-related. Treatment-related AEs led to discontinuation in 14 (6.7%) patients; the most common causes were pneumonitis in 7 (3.3%) and infusion-related reactions in 2 (1.0%), followed by myocarditis, cytokine release syndrome, myelitis, myositis, epilepsy, and organizing pneumonia in 1 patient each.
Treatment-related AEs occurring in ≥5.0% of the total study population and immune-mediated AEs and infusion-related reactions occurring in ≥1 patient
| AEs | ||||
|---|---|---|---|---|
| Grade 1 or 2 | Grade 3 | Grade 4 | Any grade | |
| Treatment-related AEs, n (%)* | ||||
| Any AE | 128 (60.9) | 23 (11.0) | 2 (1.0) | 153 (72.9) |
| Hypothyroidism | 30 (14.3) | 0 (0) | 0 (0) | 30 (14.3) |
| Pyrexia | 23 (10.9) | 1 (0.5) | 0 (0) | 24 (11.4) |
| Rash | 23 (11.0) | 0 (0) | 0 (0) | 23 (11.0) |
| Fatigue | 22 (10.5) | 1 (0.5) | 0 (0) | 23 (11.0) |
| Headache | 16 (7.6) | 0 (0) | 0 (0) | 16 (7.6) |
| Diarrhea | 15 (7.1) | 3 (1.4) | 0 (0) | 18 (8.6) |
| Nausea | 15 (7.1) | 0 (0) | 0 (0) | 15 (7.1) |
| Cough | 13 (6.2) | 1 (0.5) | 0 (0) | 14 (6.7) |
| Pruritus | 13 (6.2) | 0 (0) | 0 (0) | 13 (6.2) |
| Arthralgia | 11 (5.2) | 1 (0.5) | 0 (0) | 12 (5.7) |
| Infusion-related reaction | 11 (5.2) | 0 (0) | 0 (0) | 11 (5.2) |
| Neutropenia | 6 (2.9) | 5 (2.4) | 0 (0) | 11 (5.2) |
| Immune-mediated AEs and infusion-related reactions, n (%)† | ||||
| Any AE | 65 (31.0) | 5 (2.4) | 1 (0.5) | 71 (33.8) |
| Hypothyroidism | 33 (15.7) | 0 | 0 | 33 (15.7) |
| Infusion-related reactions | 11 (5.2) | 0 | 0 | 11 (5.2) |
| Pneumonitis | 10 (4.8) | 0 | 0 | 10 (4.8) |
| Hyperthyroidism | 8 (3.8) | 0 | 0 | 8 (3.8) |
| Cytokine release syndrome | 5 (2.4) | 1 (0.5) | 0 | 6 (2.9) |
| Hypersensitivity | 5 (2.4) | 1 (0.5) | 0 | 6 (2.9) |
| Colitis | 1 (0.5) | 1 (0.5) | 0 | 2 (1.0) |
| Myositis | 1 (0.5) | 1 (0.5) | 0 | 2 (1.0) |
| Myocarditis | 0 | 0 | 1 (0.5) | 1 (0.5) |
| Autoimmune thyroiditis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Iridocyclitis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Iritis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Enterocolitis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Autoimmune hepatitis | 0 | 1 (0.5) | 0 | 1 (0.5) |
| Drug hypersensitivity | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Sarcoidosis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Encephalitis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Organizing pneumonia | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Pruritus | 0 | 1 (0.5) | 0 | 1 (0.5) |
| AEs | ||||
|---|---|---|---|---|
| Grade 1 or 2 | Grade 3 | Grade 4 | Any grade | |
| Treatment-related AEs, n (%)* | ||||
| Any AE | 128 (60.9) | 23 (11.0) | 2 (1.0) | 153 (72.9) |
| Hypothyroidism | 30 (14.3) | 0 (0) | 0 (0) | 30 (14.3) |
| Pyrexia | 23 (10.9) | 1 (0.5) | 0 (0) | 24 (11.4) |
| Rash | 23 (11.0) | 0 (0) | 0 (0) | 23 (11.0) |
| Fatigue | 22 (10.5) | 1 (0.5) | 0 (0) | 23 (11.0) |
| Headache | 16 (7.6) | 0 (0) | 0 (0) | 16 (7.6) |
| Diarrhea | 15 (7.1) | 3 (1.4) | 0 (0) | 18 (8.6) |
| Nausea | 15 (7.1) | 0 (0) | 0 (0) | 15 (7.1) |
| Cough | 13 (6.2) | 1 (0.5) | 0 (0) | 14 (6.7) |
| Pruritus | 13 (6.2) | 0 (0) | 0 (0) | 13 (6.2) |
| Arthralgia | 11 (5.2) | 1 (0.5) | 0 (0) | 12 (5.7) |
| Infusion-related reaction | 11 (5.2) | 0 (0) | 0 (0) | 11 (5.2) |
| Neutropenia | 6 (2.9) | 5 (2.4) | 0 (0) | 11 (5.2) |
| Immune-mediated AEs and infusion-related reactions, n (%)† | ||||
| Any AE | 65 (31.0) | 5 (2.4) | 1 (0.5) | 71 (33.8) |
| Hypothyroidism | 33 (15.7) | 0 | 0 | 33 (15.7) |
| Infusion-related reactions | 11 (5.2) | 0 | 0 | 11 (5.2) |
| Pneumonitis | 10 (4.8) | 0 | 0 | 10 (4.8) |
| Hyperthyroidism | 8 (3.8) | 0 | 0 | 8 (3.8) |
| Cytokine release syndrome | 5 (2.4) | 1 (0.5) | 0 | 6 (2.9) |
| Hypersensitivity | 5 (2.4) | 1 (0.5) | 0 | 6 (2.9) |
| Colitis | 1 (0.5) | 1 (0.5) | 0 | 2 (1.0) |
| Myositis | 1 (0.5) | 1 (0.5) | 0 | 2 (1.0) |
| Myocarditis | 0 | 0 | 1 (0.5) | 1 (0.5) |
| Autoimmune thyroiditis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Iridocyclitis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Iritis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Enterocolitis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Autoimmune hepatitis | 0 | 1 (0.5) | 0 | 1 (0.5) |
| Drug hypersensitivity | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Sarcoidosis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Encephalitis | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Organizing pneumonia | 1 (0.5) | 0 | 0 | 1 (0.5) |
| Pruritus | 0 | 1 (0.5) | 0 | 1 (0.5) |
N = 210.
No grade 5 AEs occurred.
Immune-mediated AEs were based on a list of terms specified by the sponsor and included by the investigator, regardless of attribution to study treatment or immune relatedness.
Discussion
Treatment options are needed to improve outcomes in patients with RRcHL that has progressed after ASCT.5 With more than 2 years of follow-up, pembrolizumab continued to show effective antitumor activity (71.9%) in the overall population of patients with RRcHL and in each cohort. Importantly, responses were durable in all patients, with a median DOR of 16.5 months, and a quarter of the responders had ongoing response at database lock. The ranges for median DOR and the 95% CIs for median PFS in the 3 cohorts overlapped, suggesting that the DOR and PFS are in the same range across cohorts. Complete responders had numerically longer median DOR (NR [0.0+ to 27.0+ months]) than partial responders (10.9 months [0.0+ to 25.1+]) but had overlapping ranges. A longer duration of pembrolizumab treatment may be necessary for patients with RRcHL to achieve CR. In the current study, 63.8% of patients required 1 year or more of treatment before achieving CR. Data were comparable to those reported in prior studies with comparable cohorts.2
Pembrolizumab showed effective antitumor activity in patients with RRcHL who were BV naive and those treated with BV before or after ASCT. A direct comparison of the efficacy and safety of pembrolizumab and BV in patients with RRcHL will be performed in the ongoing phase 3 KEYNOTE-204 study (ClinicalTrials.gov, #NCT02684292) and will provide insight on the choice of treatment.9
Pembrolizumab showed promising antitumor activity, with an ORR of 75% and CRR of 50% in patients treated with a second pembrolizumab course who were evaluable for response. Strikingly, all 3 patients in cohort 2 had CR in the second course. At database cutoff, 4 patients were still on treatment, 3 had completed second-course treatment, and 3 had discontinued because of disease progression and AEs. The only immune-mediated AE that occurred in the second course was sarcoidosis in a patient who had also experienced sarcoidosis in the first course. Longer follow-up will allow better characterization of response during a second course of pembrolizumab as more patients in the current study are treated with a second course. Immune-mediated AEs occurred in only 1 patient treated with a second course of pembrolizumab.
The safety profile of pembrolizumab continued to be consistent with that of previous reports and with that of nivolumab.1,2,4 At 2 years of follow-up, no new toxicities or treatment-related deaths occurred with pembrolizumab. Similarly, no new toxicities or treatment-related deaths were reported after 1.5 years of follow-up with nivolumab.2 Low-grade hypothyroidism was the most commonly reported immune-related AE with long-term nivolumab (grades 1 and 2, 9.0%)2 and with long-term pembrolizumab (grades 1 and 2, 15.7%). Extended follow-up confirmed the acceptable safety, confirmed the robust antitumor activity, and showed durability of response of pembrolizumab in patients with RRcHL. In addition, response was generally deep and durable regardless of BV use or sequence of BV use. Thus, pembrolizumab has manageable safety and effective antitumor activity in a broad range of patients with RRcHL and may confer additional antitumor activity in patients treated with a second course.
Merck Sharp & Dohme Corp, a subsidiary of Merck & Co, Inc (Kenilworth, NJ), is committed to providing qualified scientific researchers access to anonymized patient-level data and clinical study reports from the company’s clinical trials for the purpose of conducting legitimate scientific research. The company is also obligated to protect the rights and privacy of trial participants and, as such, has a procedure in place for evaluating and fulfilling requests for sharing company clinical trial data with qualified external scientific researchers. The process includes submission of data requests to the Merck data sharing website (available at http://engagezone.msd.com/ds_documentation.php). Data will be made available for request after product approval in the US and EU or after product development is discontinued. There are circumstances that may prevent Merck from sharing the requested data.
This work was presented in part at the 60th annual meeting of the American Society of Hematology, San Diego, CA, 1-4 December 2018.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
The authors thank the patients, their families, and caregivers for participating in the study; Seth Thompson for statistical support; Victoria Fox for study team support; and Mohammed Farooqui for study oversight (Merck Sharp & Dohme Corp, a subsidiary of Merck & Co, Inc, Kenilworth, NJ).
Funding for this research was provided by Merck Sharp & Dohme Corp. Medical writing and/or editorial assistance, provided by Doyel Mitra and Matthew Grzywacz of the ApotheCom pembrolizumab team (Yardley, PA), was funded by Merck Sharp & Dohme Corp.
Thanks to the KEYNOTE-087 study group for its participation in this trial.
Authorship
Contribution: R.C., P.A., B.v.T., A.B., and C.H.M. contributed to conception, design, and planning of the study; R.C., V.R., M.A.S., J.L., E.K., A.N., A.B., and C.H.M. contributed to analysis of the data; R.C., P.A., N.A.J., P.B., H.J.L., J.R., V.R., D.M., T.P.V., A.T., B.v.T., A.B., and C.H.M. contributed to acquisition of the data; R.C., P.L.Z., P.A., J.R., V.R., D.M., T.P.V., A.T., B.v.T., M.A.S., J.L., A.N., A.B., and C.H.M. contributed to interpretation of the results; R.C., A.B., and C.H.M. contributed to drafting of the manuscript; and R.C., P.L.Z., H.J.L, P.A., N.A.J., P.B., J.R., D.M., T.P.V., A.T., B.v.T., M.A.S., J.L., E.K., A.N., A.B., and C.H.M. contributed to critically reviewing or revising the manuscript for important intellectual content.
Conflict-of-interest disclosure: R.C. reports employment, a leadership position, or an advisory role at Seattle Genetics, Pharmacyclics, Merck & Co, Inc, Genentech, Inc, and Millennium Pharmaceuticals, Inc; honoraria from Seattle Genetics; research funding from Merck & Co, Inc, Bristol-Myers Squibb, Seattle Genetics, Millennium Pharmaceuticals, Inc, and Pharmacyclics. P.L.Z. reports consulting for Verstem, Merck & Co, Inc, Eusapharma, and Sanofi; speaker fees from Verastem, Celltrion, Gilead, Janssen-Cilag, Bristol-Myers Squibb, Servier, Merck & Co, Inc, Immune Design, Celgene, Portola, Roche, Eusapharma, and Kyowa Kirin; and advisory board fees from Verastem, Celltrion, Gilead, Janssen-Cilag, Bristol-Myers Squibb, Servier, Sandoz, Merck & Co, Inc, Immune Design, Celgene, Portola, Roche, Eusapharma, and Kyowa Kirin. P.A. reports employment, a leadership position, or an advisory role at Merck Sharp & Dohme Corp, a subsidiary of Merck & Co, Inc, Kenilworth, NJ, Bristol-Myers Squibb, and Infinity Pharmaceuticals; research funding from Merck & Co, Inc, Bristol-Myers Squibb, Pfizer, Inc, Affimed, Roche, Serventa, Otsuka, and Sigma-Tau; and travel fees, gifts, and other compensation from Bristol-Myers Squibb and Merck & Co, Inc. N.A.J. reports employment, a leadership position, or an advisory role at Roche, AbbVie, Inc, and Lundbeck; honoraria from Roche, AbbVie, Inc, Lundbeck, and Seattle Genetics; research funding from Roche, AbbVie, Inc, and Lundbeck; and travel fees, gifts, and other compensation from Roche and Lundbeck. P.B. reports honoraria from Takeda France, and Bristol-Myers Squibb; consulting and advisory roles at Takeda France; and research funding from Millennium and Takeda. J.R. reports employment, a leadership position, or an advisory role at Takeda Pharmaceutical Company, Seattle Genetics, and Novartis; stock ownership or options from GlaxoSmithKline and AstraZeneca; and research funding from Takeda Pharmaceutical Company. V.R. reports honoraria from Infinity Pharmaceuticals, Bristol-Myers Squibb, Eisai, PharmaMar, and Gilead Sciences; consulting or advisory roles for Infinity Pharmaceuticals, PharmaMar, Gilead Sciences, NanoString Technologies, Incyte, Bristol-Myers Squibb, Merck & Co, Inc, Roche/Genentech, Epizyme, AstraZeneca, and Immune Design; research funding from Argenx BVBA; patents, royalties, and other intellectual property regarding trial BAY1000394 for mantle cell lymphoma; expert testimony for Servier; travel, accommodations and expenses from Roche, Bristol-Myers Squibb, and AstraZeneca; and service as principal or subinvestigator of clinical trials for AbbVie, Agios Pharmaceuticals, Amgen, Argenx BVBA, Arno Therapeutics, Astex Pharmaceuticals, AstraZeneca, Aveo, Bayer Healthcare AG, BBB Technology, BV, Blueprint Medicines, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene Corporation, Chugai Pharmaceutical Co, Clovis Oncology, Daiichi Sankyo, Debiopharm, SA, Eisai, Eli Lilly, Exelixis, Forma, Gamamabs, Genentech, Inc, GlaxoSmithKline, H3 Biomedicine, Inc, Hoffmann-La Roche AG, Innate Pharma, Iris Servier, Janssen Cilag, Kyowa Kirin Pharmaceutical Development, Inc, Loxo Oncology, Lytix Biopharma AS, Medimmune, Menarini Ricerche, Merck Sharp & Dohme, Chibret, Merrimack Pharmaceuticals, Merus, Millennium Pharmaceuticals, Nanobiotix, Nektar Therapeutics, Novartis Pharmaceuticals, Octimet Oncology, NV, Oncoethix, Onyx Therapeutics, Orion Pharma, Oryzon Genomics, Pfizer, Inc, Pharma Mar, Pierre Fabre, Roche, Sanofi Aventis, Taiho Pharma, Tesaro, Inc, and Xencor. V.R. also reports the following to his institution: as part of the Drug Development Department (DITEP): principal or subinvestigator of clinical trials for AbbVie, Aduro Biotech, Agios Pharmaceuticals, Amgen, Argenx, BVBA, Arno Therapeutics, Astex Pharmaceuticals, AstraZeneca, AstraZeneca, AB, Aveo, Bayer Healthcare, AG, Bbb Technologies, BV, Beigene, Bioalliance Pharma, Biontech AG, Blueprint Medicines, Boehringer Ingelheim, Boston Pharmaceuticals, Inc, Bristol-Myers Squibb, Bristol-Myers Squibb International Corporation, Celgene Corporation, Cephalon, Chugai Pharmaceutical Co, Clovis Oncology, Daiichi Sankyo, Debiopharm, SA, Eisai, Eli Lilly, Exelixis, Forma, Gamamabs, Genentech, Inc, Gilead Sciences, Inc, GlaxoSmithKline, Glenmark Pharmaceuticals, H3 Biomedicine, Inc, Hoffmann-La Roche, AG, Incyte Corporation, Innate Pharma, Institut de Recherche Pierre Fabre, Iris Servier, Janssen-Cilag, Janssen Research Foundation, Kura Oncology, Kyowa Kirin Pharmaceutical Development, Inc, Lilly France, Loxo Oncology, Lytix Biopharma, AS, Medimmune, Menarini Ricerche, Merck KGaA, Merck Sharp & Dohme, Chibret, Merrimack Pharmaceuticals, Merus, Millennium Pharmaceuticals, Nanobiotix, Nektar Therapeutics, Nerviano Medical Sciences, Novartis Pharmaceuticals, Octimet Oncology NV, Oncoethix, Oncomed, Oncopeptides, Onyx Therapeutics, Orion Pharma, Oryzon Genomics, Pfizer, Inc, Pharma Mar, Pierre Fabre Medicament, Plexxikon, Rigontec, GmbH, Roche, Sanofi Aventis, Sierra Oncology, Taiho Pharma, Tesaro, Tioma Therapeutics, Wyeth Pharmaceuticals France, Xencor, and Y’s Therapeutics; research grants from AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Janssen-Cilag, Merck & Co, Inc, Novartis, Pfizer, Inc, Roche, and Sanofi; and nonfinancial support (drug supplied) from AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Johnson & Johnson, Eli Lilly, Medimmune, Merck & Co, Inc, NH TherAGuiX, Pfizer, Inc, and Roche. D.M. reports honoraria from Roche Holding AG, Merck & Co, Inc, Bristol-Myers Squibb, and Takeda Pharmaceutical Company. T.P.V. reports employment, a leadership position, or an advisory role at Roche, Takeda Pharmaceutical Company, Genesis Pharmaceutical, Inc, Novartis, and Bristol-Myers Squibb; honoraria from Roche, Takeda Pharmaceutical Company, Novartis, and Bristol-Myers Squibb; and travel fees, gifts, and other compensation from Roche, Takeda Pharmaceutical Company, and Genesis Pharmaceutical, Inc. B.v.T. reports other compensation from Novartis, Takeda Pharmaceutical Company, Amgen, Celgene, and Merck Sharp & Dohme Corp. M.A.S. reports employment, a leadership position, or an advisory role at AstraZeneca, Bristol-Myers Squibb, Merck Sharp & Dohme Corp, Gilead Sciences, Inc, and Takeda Pharmaceutical Company; honoraria from AstraZeneca, Bristol-Myers Squibb, Merck & Co, Inc, Gilead Sciences, Inc, and Takeda Pharmaceutical Company; and research funding from Bristol-Myers Squibb and Bayer. J.L., E.K. and A.N. report employment at Merck Sharp & Dohme Corp. A.B. reports employment, a leadership position, or an advisory role at Merck Sharp & Dohme Corp and stock ownership in Merck Sharp & Dohme Corp and Amgen. C.H.M. reports employment, a leadership position, or an advisory role at Celgene, Genentech, Inc, Merck Sharp & Dohme Corp, and Seattle Genetics; and research funding from Pharmacyclics, Genentech, Inc, Merck & Co, and Seattle Genetics. H.J.L. and A.T. declare no competing financial interests.
Correspondence: Robert Chen, City of Hope National Medical Center, 1500 East Duarte Rd, Duarte, CA, 91010; e-mail: rwc755@gmail.com, r.chen@autolus.com.
