

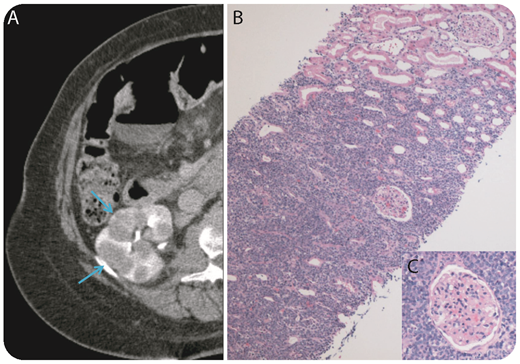
A 69-year-old woman presented to her primary care physician with an enlarging circumferential neck mass and difficulty swallowing. A bronchoscopy with fine needle aspiration was compatible with a CD10+, TdT− B-cell lymphoma with a high proliferation rate (Ki-67 > 95%). Cross-sectional imaging of her chest, abdomen, and pelvis revealed extensive disease with a large mediastinal mass and extranodal disease, including omental caking and multiple bilateral kidney masses (panel A). There was no additional lymphadenopathy in the chest, abdomen, or pelvis. Remarkably, kidney function was normal. Core biopsy of the right kidney revealed sheets of large neoplastic cells with irregular nuclei, vesicular chromatin, and a blastoid morphology, sparing the glomeruli (panel B, original magnification ×10, hematoxylin and eosin stain; panel C, original magnification ×100, hematoxylin and eosin stain). Neoplastic B cells expressed CD20 (weak), CD79a, PAX5, CD10 (weak), and BCL2by immunohistochemical stains. Fluorescence in situ hybridization analysis revealed rearrangements in MYC (59%) and BCL6 (43%) genes and translocation involving IGH-BCL2 (50%) consistent with a “triple-hit” high-grade B-cell lymphoma.
The patient is currently receiving chemotherapy with dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin. This case shows how “triple-hit” lymphoma can present atypically with limited lymphadenopathy and diffuse extranodal disease and consequently the high risk of secondary central nervous system disease.
A 69-year-old woman presented to her primary care physician with an enlarging circumferential neck mass and difficulty swallowing. A bronchoscopy with fine needle aspiration was compatible with a CD10+, TdT− B-cell lymphoma with a high proliferation rate (Ki-67 > 95%). Cross-sectional imaging of her chest, abdomen, and pelvis revealed extensive disease with a large mediastinal mass and extranodal disease, including omental caking and multiple bilateral kidney masses (panel A). There was no additional lymphadenopathy in the chest, abdomen, or pelvis. Remarkably, kidney function was normal. Core biopsy of the right kidney revealed sheets of large neoplastic cells with irregular nuclei, vesicular chromatin, and a blastoid morphology, sparing the glomeruli (panel B, original magnification ×10, hematoxylin and eosin stain; panel C, original magnification ×100, hematoxylin and eosin stain). Neoplastic B cells expressed CD20 (weak), CD79a, PAX5, CD10 (weak), and BCL2by immunohistochemical stains. Fluorescence in situ hybridization analysis revealed rearrangements in MYC (59%) and BCL6 (43%) genes and translocation involving IGH-BCL2 (50%) consistent with a “triple-hit” high-grade B-cell lymphoma.
The patient is currently receiving chemotherapy with dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin. This case shows how “triple-hit” lymphoma can present atypically with limited lymphadenopathy and diffuse extranodal disease and consequently the high risk of secondary central nervous system disease.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal