

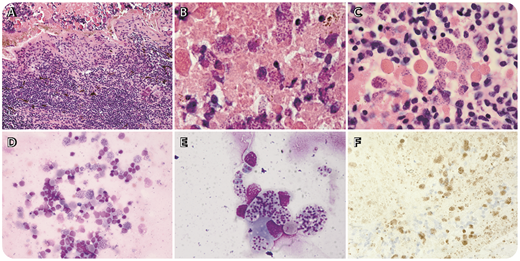
A 91-year-old woman presented with cloudy vision in her right eye for 10 months. She received empiric intravitreal antibiotics without improvement. Ophthalmoscopic examination showed significant anterior chamber vitritis and diffuse subretinal and retinal white infiltrates. Magnetic resonance imaging of her brain and orbit were negative. Vitreous bacterial cultures and polymerase chain reaction for virus were negative. Flow cytometry of vitreous fluid showed no monotypic B cells and MYD88 mutational analysis was negative. A chorioretinal biopsy was performed because of clinical suspicion for vitreous lymphoma. Histologic sections revealed necrosis and a dense infiltrate of small lymphoid cells. Numerous Toxoplasma gondii bradyzoites were found within the necrotic tissue. Cytologic preparations showed organisms surrounded by small lymphocytes, histiocytes, and neutrophils (rare). Immunohistochemistry using T gondii rabbit polyclonal antibody (Cell Marque, Rocklin, CA) confirmed the diagnosis of intraocular toxoplasmosis (panel F) (panels A-F; hematoxylin and eosin stain; original magnification: panels A,D,F: ×40; panels B,C,E: ×1000).
Diagnosis of vitreous lymphoma is challenging because of the small specimens obtained by vitreous aspiration or retinal biopsy, often requiring combined modalities including culture, cytology, and flow cytometry. This case illustrates that, in addition to lymphoma, the differential of retinal whitening and vitreous opacity includes infections with unusual organisms such as T gondii.
A 91-year-old woman presented with cloudy vision in her right eye for 10 months. She received empiric intravitreal antibiotics without improvement. Ophthalmoscopic examination showed significant anterior chamber vitritis and diffuse subretinal and retinal white infiltrates. Magnetic resonance imaging of her brain and orbit were negative. Vitreous bacterial cultures and polymerase chain reaction for virus were negative. Flow cytometry of vitreous fluid showed no monotypic B cells and MYD88 mutational analysis was negative. A chorioretinal biopsy was performed because of clinical suspicion for vitreous lymphoma. Histologic sections revealed necrosis and a dense infiltrate of small lymphoid cells. Numerous Toxoplasma gondii bradyzoites were found within the necrotic tissue. Cytologic preparations showed organisms surrounded by small lymphocytes, histiocytes, and neutrophils (rare). Immunohistochemistry using T gondii rabbit polyclonal antibody (Cell Marque, Rocklin, CA) confirmed the diagnosis of intraocular toxoplasmosis (panel F) (panels A-F; hematoxylin and eosin stain; original magnification: panels A,D,F: ×40; panels B,C,E: ×1000).
Diagnosis of vitreous lymphoma is challenging because of the small specimens obtained by vitreous aspiration or retinal biopsy, often requiring combined modalities including culture, cytology, and flow cytometry. This case illustrates that, in addition to lymphoma, the differential of retinal whitening and vitreous opacity includes infections with unusual organisms such as T gondii.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal