

We report a case of a 63-year-old patient referred to the intensive care unit for signs of tamponade. Six years earlier, she was diagnosed immunoglobulin G κ multiple myeloma (MM) with translocation (4;14) and deletion 17p, which was treated with bortezomib and dexamethasone and then lenalidomide and bendamustine after relapse. She had undergone hematopoietic stem cell transplantation (HSCT) 2 years ago, achieving a partial remission. On admission, a cardiac ultrasound showed a pericardial effusion requiring drainage. Examination of pericardial fluid showed an infiltration of atypical plasma cells of ∼15 µm with a single nucleolus, abnormal chromatin condensation, and an irregular nuclear contour (panel A; May-Grünwald Giemsa stain, original magnification ×500). Flow cytometry performed on pericardial fluid confirmed that these cells were monotypic κ plasma cells with high expression of CD38 and CD138 (panels B and C). Treatment with pomalidomide, bortezomib, and dexamethasone was started. Unfortunately, the patient died a few days later.
Although extramedullary relapse is more common after HSCT, pericardial involvement is rare, and only a few cases have been reported in the literature. Drainage of symptomatic effusions is recommended, but this condition carries a very poor prognosis in MM, and most cases are diagnosed retrospectively at postmortem examination.
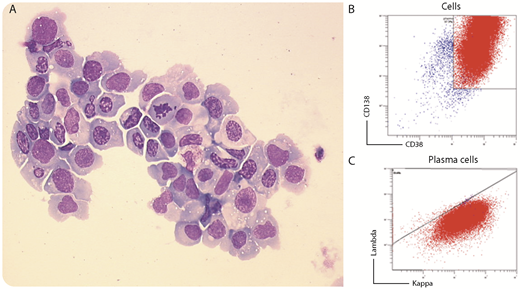
We report a case of a 63-year-old patient referred to the intensive care unit for signs of tamponade. Six years earlier, she was diagnosed immunoglobulin G κ multiple myeloma (MM) with translocation (4;14) and deletion 17p, which was treated with bortezomib and dexamethasone and then lenalidomide and bendamustine after relapse. She had undergone hematopoietic stem cell transplantation (HSCT) 2 years ago, achieving a partial remission. On admission, a cardiac ultrasound showed a pericardial effusion requiring drainage. Examination of pericardial fluid showed an infiltration of atypical plasma cells of ∼15 µm with a single nucleolus, abnormal chromatin condensation, and an irregular nuclear contour (panel A; May-Grünwald Giemsa stain, original magnification ×500). Flow cytometry performed on pericardial fluid confirmed that these cells were monotypic κ plasma cells with high expression of CD38 and CD138 (panels B and C). Treatment with pomalidomide, bortezomib, and dexamethasone was started. Unfortunately, the patient died a few days later.
Although extramedullary relapse is more common after HSCT, pericardial involvement is rare, and only a few cases have been reported in the literature. Drainage of symptomatic effusions is recommended, but this condition carries a very poor prognosis in MM, and most cases are diagnosed retrospectively at postmortem examination.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal