

A 53-year-old woman presented with fever, chills, and rigors associated with occipital headache with no localizing sign or symptoms. She had recently returned to Australia after spending 2 months in Cambodia. C-reactive protein level peaked at 120 mg/L. Initial extensive microbe cultures were negative. A whole-body computed tomography scan did not detect any infection or malignancy. As part of the work-up for fever of unknown origin, a bone marrow biopsy was performed. Her bone marrow aspirate was hypercellular with increased granulopoiesis that was left shifted. Careful examination of the trephine sample showed occasional noncaseating ring-shaped granulomas (panel A, original magnification ×10; panel B, original magnification ×40; hematoxylin and eosin stain). Monocytes and histiocytes were diffusely increased and surrounded the granulomas (panel C, original magnification ×40; CD68 immunohistochemical stain). A sample with Ziehl-Neelsen stain was negative and there was no malignant infiltration. Although epithelioid/ring granulomas are characteristic of Q fever, they are not pathognomonic of Q fever and have been reported in patients with viral infections, brucellosis, leishmaniasis, and lymphomas. Q fever serology demonstrated seroconversion consistent with recent infection.
Q fever is the result of an infection by Coxiella burnetii, a gram-negative intracellular bacteria, and patients usually present with protracted severe flu-like symptoms. Our patient was started on treatment with doxycycline, which resulted in resolution of her symptoms.
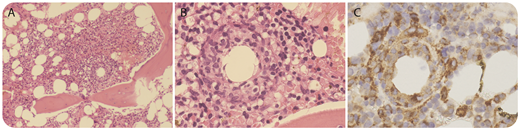
A 53-year-old woman presented with fever, chills, and rigors associated with occipital headache with no localizing sign or symptoms. She had recently returned to Australia after spending 2 months in Cambodia. C-reactive protein level peaked at 120 mg/L. Initial extensive microbe cultures were negative. A whole-body computed tomography scan did not detect any infection or malignancy. As part of the work-up for fever of unknown origin, a bone marrow biopsy was performed. Her bone marrow aspirate was hypercellular with increased granulopoiesis that was left shifted. Careful examination of the trephine sample showed occasional noncaseating ring-shaped granulomas (panel A, original magnification ×10; panel B, original magnification ×40; hematoxylin and eosin stain). Monocytes and histiocytes were diffusely increased and surrounded the granulomas (panel C, original magnification ×40; CD68 immunohistochemical stain). A sample with Ziehl-Neelsen stain was negative and there was no malignant infiltration. Although epithelioid/ring granulomas are characteristic of Q fever, they are not pathognomonic of Q fever and have been reported in patients with viral infections, brucellosis, leishmaniasis, and lymphomas. Q fever serology demonstrated seroconversion consistent with recent infection.
Q fever is the result of an infection by Coxiella burnetii, a gram-negative intracellular bacteria, and patients usually present with protracted severe flu-like symptoms. Our patient was started on treatment with doxycycline, which resulted in resolution of her symptoms.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal