

A 66-year-old man from the Dominican Republic presented to the Myeloproliferative Neoplasms Clinic at Mount Sinai with a 10-year history of untreated JAK2V617F-positive primary myelofibrosis (PMF). Bone marrow biopsy confirmed a hypercellular bone marrow with granulocytic hyperplasia, clusters of pleomorphic megakaryocytes, and diffuse reticulin and collagen fibrosis (MF3) (panel A, hematoxylin and eosin stain; panel B, reticulin stain; panel C, trichrome stain; original magnification, ×400). Concurrent with progressive symptomatic splenomegaly and transfusion dependent anemia, the patient developed refractory tophaceous gout of the bilateral hands, causing significant and disabling deformity (panels D-E). Refractory gout refers to those patients who have progressive disease with ongoing symptoms and failure to achieve a target serum uric acid level less than 6 mg/dL. At the time of presentation at our clinic, the patient’s uric acid level was 8.7 mg/dL (4.0-9.0 mg/dL) despite receiving the maximal renal adjusted dose of allopurinol. Ruxolitinib therapy for PMF-related splenomegaly and constitutional symptoms was initiated and pegloticase administered to address the gouty arthritis. The patient had a dramatic response to pegloticase, with significant improvement in hand swelling and deformity (panels F-G), and his uric acid levels decreased to 1.0 mg/dL.
Secondary gout has been described in the proliferative phase of PMF attributed to increased hematopoietic cell turn over; however, refractory gout in the setting of untreated PMF is rare.
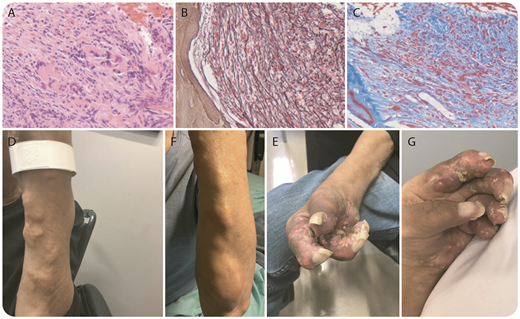
A 66-year-old man from the Dominican Republic presented to the Myeloproliferative Neoplasms Clinic at Mount Sinai with a 10-year history of untreated JAK2V617F-positive primary myelofibrosis (PMF). Bone marrow biopsy confirmed a hypercellular bone marrow with granulocytic hyperplasia, clusters of pleomorphic megakaryocytes, and diffuse reticulin and collagen fibrosis (MF3) (panel A, hematoxylin and eosin stain; panel B, reticulin stain; panel C, trichrome stain; original magnification, ×400). Concurrent with progressive symptomatic splenomegaly and transfusion dependent anemia, the patient developed refractory tophaceous gout of the bilateral hands, causing significant and disabling deformity (panels D-E). Refractory gout refers to those patients who have progressive disease with ongoing symptoms and failure to achieve a target serum uric acid level less than 6 mg/dL. At the time of presentation at our clinic, the patient’s uric acid level was 8.7 mg/dL (4.0-9.0 mg/dL) despite receiving the maximal renal adjusted dose of allopurinol. Ruxolitinib therapy for PMF-related splenomegaly and constitutional symptoms was initiated and pegloticase administered to address the gouty arthritis. The patient had a dramatic response to pegloticase, with significant improvement in hand swelling and deformity (panels F-G), and his uric acid levels decreased to 1.0 mg/dL.
Secondary gout has been described in the proliferative phase of PMF attributed to increased hematopoietic cell turn over; however, refractory gout in the setting of untreated PMF is rare.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal