

Abstract
INTRODUCTION
The incidence of secondary cancer (SC) in patients with myeloproliferative neoplasms (MPN) is high and comparable to that of thrombosis. However, the identification of patient subgroups that might be at increased susceptibility of developing SC has not been systematically addressed. We report here the results of an international case-control study (MPN-K) aimed at comparing the frequency of exposure to possible causes of SC in patients with classical MPN, polycythemia vera (PV), essential thrombocythemia (ET) and myelofibrosis (MF).
METHODS
This European Leukaemia Network (ELN) study reports MPN patients from 28 sites of 5 European countries and Israel, diagnosed in the period from 2000 to 2016. Cases were MPN patients with concomitant diagnosis of a non-myeloid SC (n=15) or its presentation during the course of the disease (n=412). Controls were MPN patients cancer-free, matched to the paired case for sex, age (±5 years), date of MPN diagnosis (±5 years), and MPN disease duration (±6 years). A multivariable conditional logistic regression model was used to estimate the effect of selected variables on total SC risk and in different types of SC.
RESULTS
Among 1,259 MPN patients, there were 427 cases and 832 matched controls. Cases presented melanoma (n=20; 4.7%), non-melanoma skin cancer (n=69; 16.2% - basal/squamous cell carcinoma), non-skin solid cancer (n=290; 67.9%) including breast, ovary/uterus, colorectal, upper gastrointestinal, liver/pancreas, lung, prostate/urinary, other and lymphoproliferative diseases (n=48; 11.2%) including multiple myeloma, chronic lymphocytic leukemia, low and high grade B- and T-lymphoma.
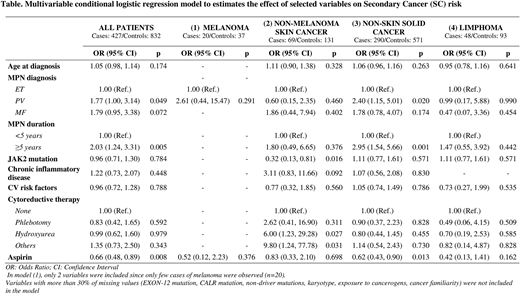
At diagnosis, there were slightly more patients with PV among SC cases (n= 152; 35.6%) than controls (n=256; 30.8%), while conversely there were slightly less ET patients among cases (n=196; 45.9%) than controls (n=426; 51.2%). Cases and controls presented similar proportion of MF diagnosis (n=79 cases, 18.5% and 150 controls, 18.0%). Driver mutations (JAK2 V617, EXON-12, CALR, MPL), non-driver mutations and abnormal karyotype were equally represented in cases and controls. Other variables such as cardiovascular risk factors, exposure to cancerogens, family history of cancer and chronic inflammatory diseases were reported with similar frequency in cases and controls.
After MPN diagnosis, exposure to first and other lines of treatments until the index event, with Phlebotomy (n=193; 15.3%), Hydroxyurea (n=814; 64.7%), Anagrelide (n=14; 1.1%), Interferon (n=30; 2.4%), Pipobroman (n=8; 0.6%), Busulphan (n=13; 1.0%), Ruxolitinib (n=11; 0.9%), was similar in the two groups except for aspirin that was used less frequently (p=0.043) in cases (n=320; 74.9%) compared to controls (n=664; 79.9%). In particular, the lower use of aspirin was circumscribed to non-skin solid tumors. A multivariable analysis was carried out in all patients and stratified by different type of tumors (Table). In non-skin solid cancers, the time to exposure of the MPN disease > 5 years (OR=2.95; 95% CI 1.54-5.66, p=0.001) and the PV phenotype (OR=2.40, 95% CI 1.15-5.01, p=0.020) were more burdened by the incidence of events than the reference ET group. No difference in SC risk was found for MF patients compared to patients with ET.
Interestingly, the independent protective role of aspirin retained its statistical significance only in non-skin SC. In non-melanoma skin cancer, multivariable analysis revealed that the presence of JAK2 mutation was less associated with SC (OR=0.32, 95% CI 0.13-0.81, p=0.016) and confirmed that exposure to HU and other cytotoxic agents was associated with a significantly higher risk of SC (OR=6.00, 95% CI 1.23-29.28, p=0.027 and OR=9.80, 95% CI 1.24-77.78, p=0.031, respectively). This finding was not seen in non-skin SC and in lymphoma.
CONCLUSION
The considered clinical and biological features, at MPN diagnosis, were not different in cases with SC and controls. During the course of the disease, three factors significantly and independently affected the risk of SC in these MPN patients: 1) patients with PV had a 77% higher risk than those with ET, 2) patients with MPN duration of more than 5 years had a twice higher risk than those with lower duration, 3) for the first time, we documented that in non-skin solid cancers, aspirin treatment reduced SC risk of 38%. Exposure to HU and other cytoreductive drugs was confirmed as a risk factor for non-melanoma skin cancer.
Palandri:Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Marchetti:Gilead: Consultancy; takeda: Speakers Bureau; amgen: Speakers Bureau; janssen: Speakers Bureau. Griesshammer:Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal