

Abstract

Introduction: For transplant-ineligible patients (pts) with newly diagnosed MM, the efficacy of VMP was established in the phase 3 VISTA trial. To reduce toxicity of VMP, twice-weekly bortezomib (V) was limited to the first cycle or completely replaced with once-weekly V in subsequent VMP-based trials (GIMEMA MM-03-05, GEM2005MAS65, and ALCYONE), and recent guidelines have recommended a less-intensive VMP schedule (Moreau P, et al. Ann Oncol 2017. 28[suppl_4]:iv52-iv61). In the absence of clinical trials directly comparing the VISTA VMP dosage regimen with modified VMP regimens, a matching adjusted indirect comparison (MAIC) provides a means to compare absolute treatment effects across diverse populations while minimizing the risk of bias associated with a naive indirect comparison. The objective of the present analysis is to compare the efficacy and safety of a modified dosing schedule of V in VMP-based regimens vs the dosing schedule established in VISTA for transplant-ineligible MM.
Methods: Primary analysis was a comparison of the VMP schedule of VISTA vs modified VMP schedules pooled from the ALCYONE (once-weekly V during Cycles 2-9) and GIMEMA MM-03-05 trials; only the once-weekly V schedule (Cycles 1-9) from GIMEMA MM-03-05 (GIMEMA-QW) was included in this analysis. GEM2005MAS65 was excluded from the primary analysis because there was no control arm without maintenance (all patients received V-based maintenance after VMP). The supplemental analysis was a comparison of VISTA vs pooled modified VMP schedules from all 3 trials.
Individual pt-level data (IPD) were obtained from the sponsor for the VISTA and ALCYONE trials, and a published validated method was used to reconstruct IPD for both progression-free survival (PFS) and overall survival (OS) of the GIMEMA-QW and GEM2005MAS65 trials (Guyot P, et al. BMC Med Res Methodol 2012.12:9).
For each analysis, two comparisons were performed, a naive comparison and MAIC. The naive comparison made no adjustments. MAIC comparison weighted individual pts in the VISTA VMP treatment arm to match the baseline characteristics to those in the pooled VMP-modified treatment arms. Available effect modifiers and prognostic factors included age, gender, International Staging System, β2-microglobulin, albumin, serum creatinine, creatinine clearance, and cytogenetic risk. For each pt in the VISTA VMP arm, a weight was attached based on propensity scores. These weights were then used to calculate weighted outcomes.
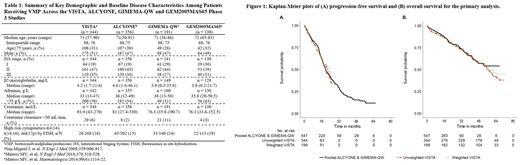
Results: A total of 344 pts received VMP in the VISTA trial and 356, 191, and 130 pts received modified VMP in the ALCYONE, GIMEMA-QW, and GEM2005MAS65 trials, respectively. Baseline demographics and clinical characteristics are provided in Table 1.
The primary analysis of VISTA vs pooled data from GIMEMA-QW and ALCYONE revealed that there were no significant differences in median PFS between VISTA (20.7 months) vs GIMEMA-QW and ALCYONE (19.6 months) in the naive comparison (HR: 0.96; 95% CI, 0.77-1.20; P = 0.74) and 23.1 vs 19.6 months in the MAIC (HR: 0.99; 95% CI, 0.76-1.30; P = 0.96; Figure 1A).
Similarly, there were no significant differences between the observed overall response rates for the VISTA schedule and the modified VMP dosing schedule for both the naive (75% vs 76%; P = 0.63) and MAIC (77% vs 76%; P = 1.00) comparisons.
For OS, survival data from ALCYONE have not yet matured, thus the median OS values for the pooled GIMEMA-QW and ALCYONE data were not reached. Median OS in VISTA was 56.4 months for the naive comparison and 58.1 months for MAIC (naive HR: 0.92; 95% CI, 0.70-1.21; P = 0.54; MAIC HR: 0.94; 95% CI, 0.68-1.28; P = 0.68; Figure 1B).
For safety, incidences of peripheral neuropathy were significantly reduced with the modified VMP dosing schedule compared with the VISTA schedule for both the naive (all-grade: 32% vs 47%; P <0.0001; Gr. 3/4: 4% vs 13%; P <0.0001) and MAIC (all-grade: 32% vs 48%; P <0.0001; Gr. 3/4: 4% vs 11%; P = 0.001) comparisons.
The supplemental analysis showed consistent results to the primary analysis for both efficacy and safety outcomes.
Conclusions: As naive, indirect comparisons are prone to bias due to patient heterogeneity between studies, a MAIC can provide useful insights for clinicians and reimbursement decision-makers on the relative efficacy and safety of different treatments. Our MAIC analysis demonstrates similar efficacy of modified VMP with VISTA VMP and a potential reduction in rates of peripheral neuropathy.
San-Miguel:Sanofi: Honoraria; Novartis: Honoraria; BMS: Honoraria; Amgen: Honoraria; Celgene: Honoraria; Janssen: Honoraria; Roche: Honoraria. Mateos:Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; GSK: Consultancy, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; GSK: Consultancy, Membership on an entity's Board of Directors or advisory committees. Goldschmidt:Amgen: Consultancy, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Bristol Myers Squibb: Consultancy, Honoraria, Research Funding; Adaptive Biotechnology: Consultancy; Janssen: Consultancy, Honoraria, Research Funding; Sanofi: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Chugai: Honoraria, Research Funding; Mundipharma: Research Funding; Novartis: Honoraria, Research Funding; ArtTempi: Honoraria. Sonneveld:Amgen: Honoraria, Research Funding; BMS: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Karyopharm: Honoraria, Research Funding. Dimopoulos:Takeda: Honoraria; Janssen: Honoraria; Celgene: Honoraria; Amgen: Honoraria; Bristol-Myers Squibb: Honoraria. Heeg:Ingress-health Nederland BV: Employment, Equity Ownership, Research Funding. Hashim:Ingress Health: Employment. Deraedt:Janssen Research & Development, LLC: Employment. Hu:Janssen Research & Development, LLC: Employment. Lam:Janssen Global Services, LLC: Employment. He:Janssen global services: Employment.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal