

Abstract
Introduction:
Acute Lymphoblastic Leukemia (ALL) is divided into Pre-B and T phenotypes depending on the progenitor cell giving rise to the malignant clone. This disease is the most common cancer in children while rare in adults. Interestingly, higher incidence rates and poorer outcomes have been reported in patients of Latin American ethnicity. This has been attributed to higher rates of Philadelphia-Like (Ph-like) ALL and increased incidence of high risk features such as absence of hyperdiploidy and absence of t(12;21). The current data among Latinos either exclusively looks at B cell precursor (BCP) ALL or does not distinguish between subtypes. Our study sets out to better define the phenotype of this subset of patients with traditionally poor outcomes.
Methods:
Our database consisted of 825 adult patients (ages 18-85 years) diagnosed with ALL from the City of Hope Comprehensive Cancer Center in Los Angeles, California. The population in Southern California has a particularly high number of Latinos due to its proximity to Mexico and Central America. According to the 2017 United States Census, 48.6% of the Los Angeles population is of Hispanic or Latino origin. Age at diagnosis, initial WBC count, CNS involvement, imumnophenotype, cytogenetics and rate of hematopoietic cell transplantation during therapy were assessed between ethnic groups. Multivariable Logistic Regression was done to determine the features that distinguish Latino patients for Non-Hispanic Whites.
Results:
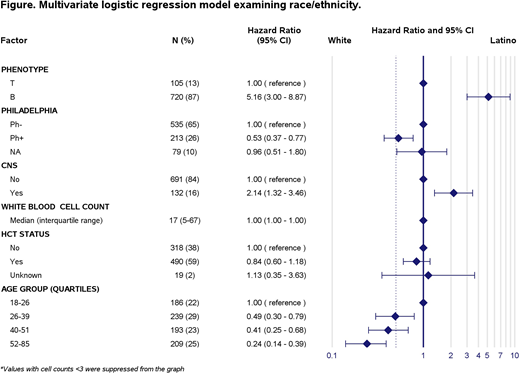
57.4% of the patients were Latinos and 42.6% were Non-Hispanic Whites (NHWs), a distribution unique to the Los Angeles area and consistent with US census population data. BCP ALL was more common in Latinos when compared to NHWs with a Hazard Ratio of 5.13 (95% CI between 2.97-8.87). The presence of the t(9;22) or Philadelphia chromosome (Ph+) was more common in NHW patients. The Hazard Ratio for Ph+ ALL in NHWs was 0.53 (95% CI between 0.37-0.77) CNS involvement was more common in Latino patients and MLL was the only cytogenetic abnormality less common in NHWs. Normal Karyotype (NK), Complex and Others were all more common in Latino patients. No difference was found between WBC counts of Latinos and NHW. (Fig. 1).
Discussion:
ALL has been shown to have higher rates in the Latino population. Our results among adults ages 18-85 years old, demonstrated that this difference can be attributed to higher incidence of BCP ALL and not T-cell among Latinos. This is consistent with the previously reported higher rate of Ph-Like ALL and distinct molecular aberrations among Latinos. Our data shows that the rate of Ph+ ALL is higher in NHWs when compared to Latinos. This is a very interesting finding as the presence of Ph+ ALL and Ph-like ALL are mutually exclusive. Associations have been previously reported between Ph-like ALL and Latin American ethnicity. Although there are types of ALL that are neither Ph+ nor Ph-like this finding suggests a higher incidence of Ph-like ALL in Latinos. At the present time, standard cytogenetics do not include CRLF2, IKZF1 and other mutations found in Ph-like ALL. Complex cytogenetics and CNS involvement, both factors associated with poor prognosis, are most likely to present in a Latino patient. While the precise mechanism is unknown, our findings further support the hypothesis that a unique genetic fingerprint has led to development and outcomes of Ph-like ALL in Latinos. It is evident that this subset of unfavorable BCP ALL population needs special attention. More studies are imperative to further elucidate the mechanism behind Ph-like ALL and pinpoint the risk factors in the Latino population.
Douer:Spectrum: Consultancy; Amgen: Membership on an entity's Board of Directors or advisory committees; Pfizer: Honoraria; Jazz Pharmaceuticals: Consultancy; Gilled Sciences, Inc: Consultancy; Shire: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal