

Abstract
Introduction:
The role of autologous hematopoietic stem cell transplantation (auto-HCT) in the management of patients with Waldenström Macroglobulinemia (WM), a rare, indolent lymphoma, has not been established. We had previously published our experience with auto-HCT in a small cohort of WM patients1. Here, we present an updated analysis of auto-HCT with a larger cohort of WM patients.
Methods and study population:
The study cohort was comprised of 29 patients who underwent high-dose chemotherapy and auto-HCT at MD Anderson Cancer Center (MDACC). The Kaplan-Meier method was used to create survival curves. Overall survival (OS) was defined as the duration from date of transplant to death or last date of follow-up in living patients. Progression-free survival (PFS) was defined as the duration from date of transplant to either progressive disease or death, whichever occurred first.
Results:
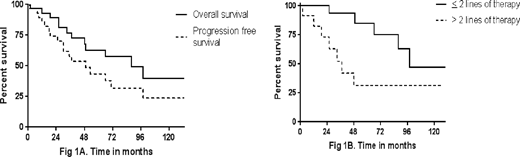
Median age at auto-HCT was 60 (range, 43-75 years). Eight patients (28%) had concurrent light chain amyloidosis (AL). Of the five patients who had MYD88 testing completed, 3 were positive for the MYD88 mutation. Additionally, of these 3 patients, 2 were also positive for CXCR4 mutation. Patients received a median of 2 lines (range 1-6) of therapy prior to auto-HCT; 3(10%) patients had primary refractory disease, 8(28%) were in first remission, and 18 (62%) had relapsed disease. Median time from transplant to last follow-up for the surviving patients was 5.3 years. Preparative regimens received by the patients were: Melphalan (n=20), BEAM-R (n=2), Busulfan/Melphalan (n=1), Cyclophosphomaide/Etoposide/total body irradiation (n=1), Thiotepa/Busulfan/Cyclophosphamide (n=1), and Carmustine/Thiotepa (n=1). Three patients further went on to receive allogeneic transplant either after relapse from auto-HCT or due to disease transformation to aggressive lymphoma. Twenty-eight patients achieved engraftment with a median time to neutrophil engraftment of 11 days (range, 10-15 days). One patient suffered primary graft failure due to progression of disease and died 84 days after transplant. Non-relapse mortality was 3.4% at 1 year. All patients were eligible for response evaluation. The median OS from diagnosis was 12.2 years. Overall response rate was 96%: complete response (n=8, 27.6%), very good partial response (n=5, 17.3%), partial response (n=15, 51.7%), and progressive disease (n=1, 3.4%). PFS and OS at 5 years were 43.3% and 62.9%, respectively. Median PFS and OS from auto-HCT were 4.1 and 7.3 years (Fig. 1A). The median OS from auto-HCT in first remission + primary refractory and relapsed disease was 8.2 years and 4.1 years, respectively.16 patients were alive at the time of censoring while 13 patients had died. Causes of death include relapsed disease (n=6), secondary malignancy (n=2), infection (n=1), chronic graft-versus-host disease (n=1), and unknown (n=3). 8 patients (28%) were positive for concurrent AL amyloidosis. The sites of amyloid involvement were kidneys (n=2), lungs (n=1), bone marrow (n=1), heart(n=1), lymph nodes(n=1), gastrointestinal tract (n=1) and subcutaneous fat aspirate(n=5). The median overall survival for patients with amyloid involvement (n=8) was 12 years. On univariate analyses, the number of chemotherapy regimens prior to transplant (≤ 2 vs >2 lines) was the strongest predictor of overall survival (p=0.03, HR 0.3, CI: 0.09-0.9, log-rank) and PFS (p=0.001, HR 0.24, CI: 0.07-0.85, log-rank). The median PFS in patients with ≤ 2 lines and > 2 lines of therapy was 71 months versus 19 months, respectively (Fig. 1B).
Conclusion:
Auto-HCT is safe and feasible in selected patients with WM, with a high response rate and durable remission even in patients with relapsed or refractory disease.
References:
Krina Patel et.al. Autologous Stem Cell Transplantation in Waldenstrom's Macroglobulinemia. Blood 2012 120:4533;
Thomas:Celgene: Research Funding; Bristol Myers Squibb Inc.: Research Funding; Acerta Pharma: Research Funding; Array Pharma: Research Funding; Amgen Inc: Research Funding. Lee:Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees; Adaptive Biotechnologies Corporation: Consultancy; Amgen: Consultancy, Membership on an entity's Board of Directors or advisory committees; Chugai Biopharmaceuticals: Consultancy; Takeda Oncology: Consultancy, Membership on an entity's Board of Directors or advisory committees; Kite Pharma: Consultancy, Membership on an entity's Board of Directors or advisory committees. Orlowski:Takeda: Consultancy; Celgene: Consultancy; Spectrum Pharma: Research Funding; Janssen: Consultancy; Kite Pharma: Consultancy; Sanofi-Aventis: Consultancy; BioTheryX: Research Funding; Amgen: Consultancy, Research Funding; Bristol-Myers Squibb: Consultancy. Champlin:Otsuka: Research Funding; Sanofi: Research Funding. Patel:Poseida Therapeutics, Inc.: Research Funding; Takeda: Research Funding; Abbvie: Research Funding; Celgene: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal