

Abstract

Background: Haploidentical (Haplo) hematopoietic cell transplantation (HCT) provides an alternative option for patients without HLA-matched donor. GVHD, engraftment failure, and infectious complications continue to be the main causes of non-relapse mortality (NRM). We hypothesized that selective depletion of TCRαβ+ and CD45RA+ naïve T cells subset will permit hematopoietic engraftment, while effectively reducing GVHD, and provide improved donor immune reconstitution through adoptive transfer of donor's mature NK and γδ T cells and CD45RA- memory T cells.
Methods: GCSF +/- plarixefor (N=13) mobilized PBSC apheresis product were divided into two fractions in 9:1 ratio, and depleted using CliniMACS device after labeling with TCRαβ and CD45RA reagents (Miltenyi Biotec, Bergish-Gladbach, Germany), respectively. The conditioning regimen consisted of total nodal irradiation 6 - 7.5 Gy over 3 equal fractions, 160 mg/m2 Fludarabine divided daily over 4 days, Thiotepa 10 mg/kg divided twice daily for 1 day and Melphalan 70-140 mg/m2 for 1 day. Short term GVHD prophylaxis for 30 days was given to 1 patient using MMF, 11 using tacrolimus or 2 using Sirolimus.
Results: We transplanted 20 adults (median age 42 years, range 20 - 68 ) and 3 children (age range 7-14 years) with high risk AML (n=14), ALL (n=6), MDS (n=2), myeloma (N=1). The patients were infused with TCRαβ and CD45RA depleted graft containing a median of 9.94 x 106 (range, 5.58 - 20.78) CD34+ cells/kg, 0.19 x 104 (range 0 - 8.53) CD45RA+CD3+ cells/kg, and 4.21 x 106 (range, 0.15 - 11.67) CD45RO+CD3+ cells/kg. In addition, the TCRαβ depleted graft fraction contained a median of 0.19 x 104 (range 0 - 8.53) TCRαβ+ cells/kg, and 8.87 x 106 (range 1.73 - 29.74) TCRγδ + cells/kg. All patients except 1 had engraftment of ANC > 500 cells/µL at a median of 11 day (range, 8 - 19) and PLT > 20,000 cells/µL at a median of 12 day (range, 7 - 19). Complete donor chimerism was seen at the time of engraftment in all patients with primary engraftment. Only 1 patient experienced primary graft failure. There was no secondary graft failure.
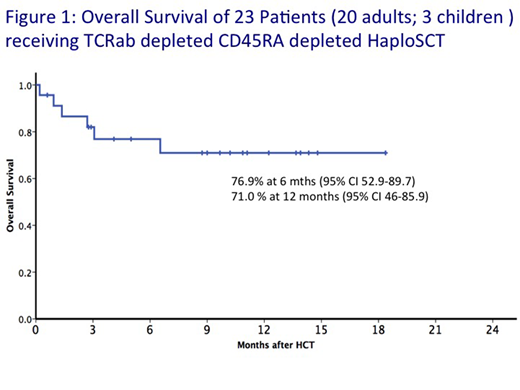
Eleven patients developed acute GVHD of grade II-IV, with the day 100 cumulative incidence (C.I.) of acute GVHD of Gd II-IV, and Gd III-IV of 50% (95% CI 27.3 - 69.0%) and 17.9 % (95% CI 5.3- 36.4%), respectively. One patient experienced chronic GVHD. Day 180 C.I. of NRM and relapse were 23.9 % (95% 8.3-43.9%) and 5.6 % (95% CI 0.3-23.3%), respectively. NRM was attributed to aGVHD in 3 of the 6 deaths. Viral reactivation included CMV (n=7), HHV6 (N=4), EBV (N=3) and adenovirus (N=2), with no fatal viral infection occurred within 100 days. Two patients had fatal blood stream infection within 100 days. With a median follow up of 306 days (range 18 - 551 days) in surviving patients, the 6 month and 1 year overall survival (OS) were 76.9% (95% CI 52.9-89.7%) and 71 % (95% CI 46-85.9%), respectively. (Figure 1).
Conclusions: Our preliminary results suggest that RIC haplo-HCT with TCRαβ and CD45RA+ depleted grafts allows successful allograft in high-risk patients lacking a suitable matched donor. NRM due to GVHD remains the major obstacle for the successful HCT. Fine adjustment of T cell dose with short course of immunosuppressant may reduce GVHD while preserving antitumor and antimicrobial immunocompetence.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal