

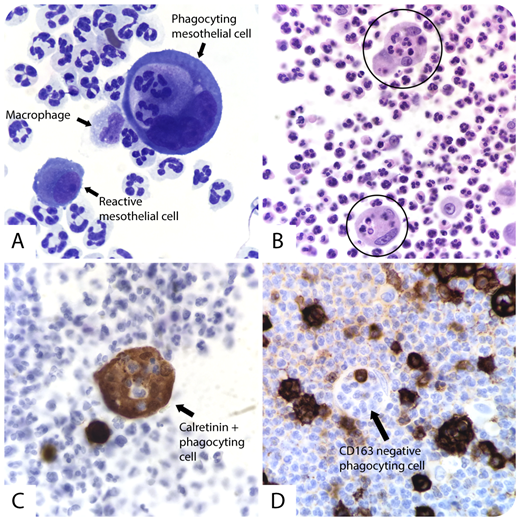
A 96-year-old man was brought to the emergency department for confusion and a 1-week history of nonproductive increasing cough. His temperature was 38.94°C, blood pressure 92/40 mm Hg, heart rate 76 beats/min, respiratory rate 26 breaths/min, and pulmonary examination revealed rales in the bases. Significant laboratory results revealed a white blood cell count of 23 000 × 109/L and glucose 159 mg/dL. The patient was admitted and empiric antibiotics were initiated for suspected septic shock secondary to pneumonia. A chest radiograph and subsequent ultrasound showed a right lower lobe infiltrate and a moderate right pleural effusion. A thoracentesis was performed and the pleural fluid was found to be straw-colored and hazy with a red blood cell count of 1400/mcL and a white blood cell count of 19 000 × 109/L. Microscopic examination of the pleural fluid revealed mostly neutrophils and occasional reactive and large multinucleated mesothelial cells demonstrating active phagocytosis of neutrophils.
Previous studies have reported that after an inflammatory stimulus, mesothelial cells can rarely express macrophage markers and possibly differentiate into phagocytic macrophage-like cells (panel A: original magnification ×100, Papanicolaou stain; panel B: original magnification ×100, hematoxylin and eosin stain; panel C: original magnification ×100, calretinin; panel D: original magnification ×100, CD163). After 10 days, the patient showed clinical improvement and was discharged with oral antibiotic treatment.
A 96-year-old man was brought to the emergency department for confusion and a 1-week history of nonproductive increasing cough. His temperature was 38.94°C, blood pressure 92/40 mm Hg, heart rate 76 beats/min, respiratory rate 26 breaths/min, and pulmonary examination revealed rales in the bases. Significant laboratory results revealed a white blood cell count of 23 000 × 109/L and glucose 159 mg/dL. The patient was admitted and empiric antibiotics were initiated for suspected septic shock secondary to pneumonia. A chest radiograph and subsequent ultrasound showed a right lower lobe infiltrate and a moderate right pleural effusion. A thoracentesis was performed and the pleural fluid was found to be straw-colored and hazy with a red blood cell count of 1400/mcL and a white blood cell count of 19 000 × 109/L. Microscopic examination of the pleural fluid revealed mostly neutrophils and occasional reactive and large multinucleated mesothelial cells demonstrating active phagocytosis of neutrophils.
Previous studies have reported that after an inflammatory stimulus, mesothelial cells can rarely express macrophage markers and possibly differentiate into phagocytic macrophage-like cells (panel A: original magnification ×100, Papanicolaou stain; panel B: original magnification ×100, hematoxylin and eosin stain; panel C: original magnification ×100, calretinin; panel D: original magnification ×100, CD163). After 10 days, the patient showed clinical improvement and was discharged with oral antibiotic treatment.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal