

Abstract

Iron overload (IO), primarily related to multiple red blood cell transfusions, is a relatively common complication in allogeneic hematopoietic stem cell transplant (allo-HSCT) recipients. Elevated pre-transplant ferritin level, a surrogate marker of iron overload, was demonstrated to be an important cause of mortality and morbidity in patients who have undergone allo-HSCT. Excessive iron accumulation results in tissue damage and organ failure, mainly as a result of the generation of free radicals that cause oxidative damage and organ dysfunction. Iron chelators have been widely used leading to normalisation for ferritine level and lower IO-related complications. As iron has a fundamental role in cell survival affecting pathways involved in DNA synthesis, cell differentiation, and apoptosis, some studies evaluated the anti-proliferative activity of iron chelators in cancer and leukemia patients on disease recurrence. The objective of this study was to determine at a first time the impact of serum ferritin level measured at time of allogeneic HSCT in adult patients with hematological disorders on the different outcomes and to investigate at a second time the role of iron chelation on relapse incidence. We included 158 patients, 100 males and 58 females with a median age of 45 years (18-67) who underwent allo-HSCT between 2002 and 2010. There were 83 acute myeloid leukemias, 10 chronic myeloid leukemias, 11 myelodysplastic syndromes, 7 myeloproliferative disorders, 19 myelomas, 9 non-Hodgkin lymphomas, 6 Hodgkin diseases, 5 aplastic anemias and 3 hemoglobinopathies. Sixty-seven (42%) patients were sex mismatched (F→M:37; M→F:30); for ABO compatibility, 61% were compatible, 18% had minor incompatibility and 21% had major incompatibility. Concerning the HSCT procedures, 60 patients (38%) received peripheral blood stem cell and 98 (62%) received bone marrow from 97 (61%) HLA related donors [matched, n=76; mismatched, n=21], and 61 (39%) HLA unrelated donors [matched, n=36; mismatched, n=25] after myeloablative [n=64, (41%)] or reduced intensity conditioning [n=94, (59%)]. At transplantation, 91 (58%) were in complete remission (CR) or chronic phase [CR1: n=61 (67%); ≥CR2: n=30 (33%)]. The median serum ferritin level at HSCT was 1327 microg./l (26-14136); 31(20%) patients had a level 26-500, 33 (21%) had a level 500-2500, and 94 (59%) >2500. There was no significant correlation between the different ferritin levels, disease kind and status at HSCT. After transplantation, 23 patients received iron chelating agents after a serum ferritin level of 1000 microg/l and stopped when the level decreased below 1000. The cumulative incidence of acute GVHD ≥ II at 3 months was 14% (11-16.5) with 10.5% (8-13) for grade III and 7% (5-9) for grade IV; the 1 year cumulative incidence of limited and extensive chronic GVHD were 4% (2-6) and 12.4% (9-16) respectively. After a median follow-up of 18 months (1-106), the 5 years OS probability was 65% for patients with ferritin level below 500 microg./l, 39% for level between 500 and 2500 microg./l and 28% for level > 2500 micog./l, [Hazard ratio= 3.5 (1.5-8.1), p=0.002]; this was explained by a significant higher TRM in patients with level >2500 [Hazard ratio= 4.3 (1.02-18), p=0.04]. Interestingly, we found in multivariate analysis that patients receiving iron chelators had significantly better OS [5 years OS= 59% vs. 34% for non-chelated patients, Hazard ratio= 0.34 (0.15-0.76), p=0.008], (Figure 1a), and experienced less disease relapse [5 years relapse incidence= 18% vs. 41% for non-chelated patients, Hazard ratio= 0.22 (0.07-0.73), p=0.012], (Figure 1b). In conclusion, we confirmed the negative impact of iron overload on the outcomes allo-HSCT recipients. More importantly, we demonstrated that iron chelators have a positive impact in reducing disease relapse by the possible mechanism of iron deprivation in leukemic cells. This clinical observation needs to be confirmed by prospective randomized trials.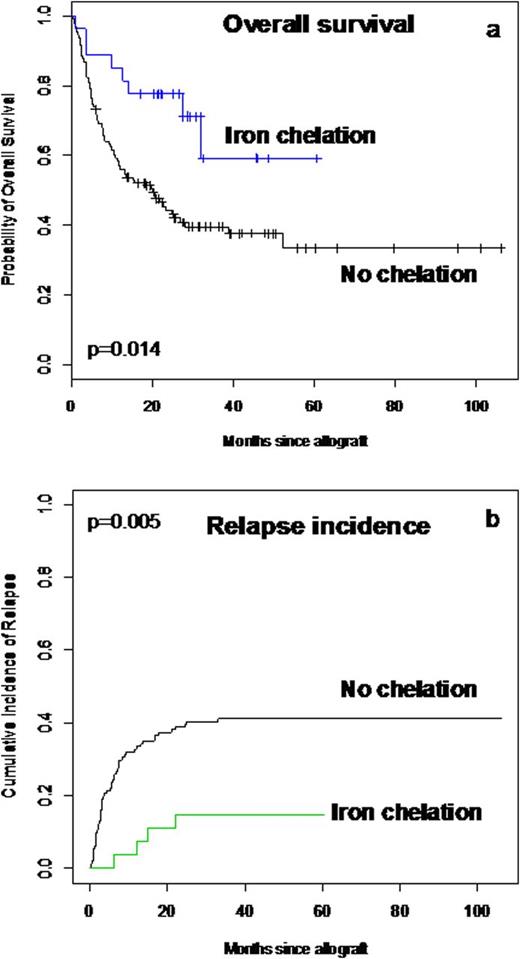 Close modal
Close modal
Figure 1

a: Overall survival probability and b: relapse incidence in patients with or without iron chelation
Figure 1
a: Overall survival probability and b: relapse incidence in patients with or without iron chelation
Disclosures:
Michallet:Novartis: Honoraria, Research Funding. Nicolini:Novartis: Consultancy, Honoraria, Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal