

Abstract
Abstract 832
Renal transplantation is the preferred therapeutic approach for end-stage renal disease. However, the chronic use of non-specific immunosuppressive agents (IS) is costly and has significant toxicities including opportunistic infection, an increased rate of malignancy, nephrotoxicity, and other end-organ damage. The induction of donor-specific tolerance would address these limitations. Bone marrow chimerism is associated with tolerance to transplanted organs and tissues. However, the toxicity associated with conventional hematopoietic stem cell transplants (HSCT), primarily graft-versus-host disease (GVHD), and the need for aggressive ablative conditioning, has limited the therapeutic application of HSCT to tolerance induction. We have identified a novel tolerogenic bone marrow cell population of CD8+/TCR− facilitating cells (FC) that enhances engraftment of bone marrow in mismatched recipients without causing GVHD. The discovery of FC is an important finding as it opens the door to employing HSCT as a viable cell-based approach for tolerance induction.
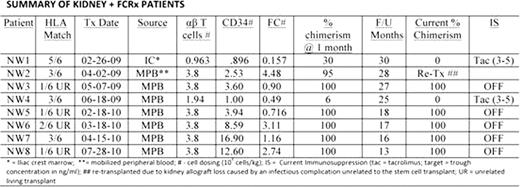
We report here the long-term follow-up for 8 HLA mismatched living donor renal transplant recipients enrolled in a tolerogenic protocol involving low-intensity conditioning (fludarabine, cyclophosphamide [50 mg/kg, day −3, +3], 200 cGy TBI) followed by HSCT and renal transplantation. Lymphocyte depleting antibody therapy was not employed. Patients received a living donor kidney transplant on day 0, followed by infusion of cryopreserved FC-enriched donor-derived CD34+ HSC (FCRx) on day +1 (0.49–4.48 × 106 FC/kg recipient body weight) and a calculated dose of T cells (Table). All subjects were discharged by post-operative day 3 and managed as outpatients. Maintenance IS consisted of tacrolimus and MMF without steroids. Weaning of immunosuppression was designed to occur over a one-year period. At 6 months, if chimerism was present and renal function and biopsy normal, the MMF was discontinued; at 9 months the tacrolimus was decreased to trough levels of 3 to 5; and at 12 months, tacrolimus was discontinued. Characteristics and degree of HLA mismatch are shown in the table.
The patients are now 13 to 30 months post-transplant. All patients demonstrated peripheral blood macrochimerism post-transplant, ranging from 6% to 100% at 1 month by STR molecular analysis. No patient developed acute GVHD, showed evidence of engraftment syndrome, or has developed evidence of chronic GVHD. Chimerism was lost in two of the patients at 3 and 6 months post-transplant (NW 1 and 4). These subjects received an FCRx containing the fewest numbers of FC. Renal allograft loss occurred in one patient who developed sepsis and myelosuppression following an atypical viral infection 2 months post-transplant. He was successfully rescued with banked autologous HSCT. He was subsequently re-transplanted. The seven remaining patients demonstrate donor-specific hyporesponsiveness. Five have been successfully withdrawn entirely from IS, with one patient now off all IS for 15 months (30 months post-transplant). Four of these five subjects had mismatched unrelated (UR) donors (Table). None developed anti-donor antibody by flow crossmatch. Adverse events have included single dermatome herpes zoster reactivation in 2 patients which resolved. No clinically significant CMV or polyoma viral infections have occurred.
Low intensity conditioning in conjunction with FC-enriched HSCT can safely achieve high level, durable donor chimerism in unrelated and related HLA-mismatched kidney transplant recipients without acute or chronic GVHD. This is associated with stable renal function and successful IS withdrawal.
Tollerud:Regenerex, LLC: Equity Ownership. King:Regenerex, LLC: Employment. Ildstad:Regenerex, LLC: Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal