

Abstract
Abstract 4124
Most patients (pts) undergoing high-dose therapy with melphalan 200 mg/m2 (HDM) and autologous transplant for multiple myeloma (MM) develop disease recurrence. The optimal salvage treatment including autologous (auto-) and allogeneic (allo-) hematopoietic stem cell transplantation (SCT) as consolidation therapy for these patients is not yet defined.
We performed a retrospective analysis of 116 pts with MM treated in our institution between 1999 and 2005. Inclusion criteria were relapse after auto-SCT (n=88) or failure of induction treatment (n=28) and age ≤ 65 years. Re-induction was performed with TCED (thalidomide, cyclophosphamide, etoposide and dexamethasone (Möhler et al, Blood 2001). Seventy-one pts (median age, 59 yrs) received auto-SCT (auto-group) after HDM followed by maintenance therapy with thalidomide or interferon-alpha in 42 pts. Forty-five pts (allo-group, median age, 53 yrs) underwent a reduced-intensity allo-SCT (related in 24 pts), mostly using conditioning with 2 Gy total body irradiation and fludarabine. Thirty-eight pts received an auto-allo-tandem-SCT (Maloney, Blood 2003) and 7 pts have been directly transplanted after TCED.
Statistical analysis was done using the two-stage test of Qiu & Sheng (JRSS Ser. B 2008) to compare two possibly crossing survival curves. Extended Cox proportional hazards regression models were applied to allow for time-varying differences between the two SCT groups.
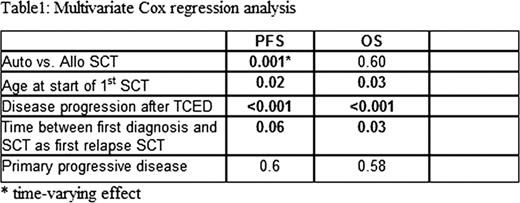
Estimated median follow-up after start of TCED was 95 months. All pts received a median number of 3 TCED cycles for re-induction therapy. 64 of 116 pts (55%) showed at least a PR after TCED chemotherapy (CR in 3 pts). TRM was 17% after 2 years in the allo-group and differed significantly from the auto-group (3%, p=0.02). More CR were achieved after allo-SCT compared to auto-SCT (17 vs. 4 pts., p<0.001). Median overall survival (OS) was 26 months for the auto group and 23 months for the allo group (Figure 1, p=0.16). Median progression-free survival (PFS) was 12 months for both groups but crossing hazards were observed (Figure 2, p=0.03, two-stage test of Qiu & Sheng). The results of multivariate regression analysis for OS and PFS including age at relapse-SCT, response to TCED, time between first diagnosis until first relapse-SCT and primary progression are shown in table 1.


In the allo group, there was no OS or PFS difference between related and unrelated donors (multivariate analysis). Cumulative incidence of chronic GvHD was 73% (53% extensive). Patients with chronic GvHD showed a better OS and PFS than pts without (univariate analysis, both p<0.01).
To our knowledge, this is the first analysis in a large number of patients with a long follow-up comparing allo with auto SCT in 1st myeloma relapse which were treated uniformly with TCED therapy for re-induction. Main problem was MM recurrence. However, younger pts with disease response after TCED and longer time from first diagnosis to first SCT after relapse profit best from TCED and this transplant approach. Most interestingly, disease control is better after allo compared to auto SCT in univariate and multivariate analysis leading to a PFS of about 20% after 4 years. In our opinion, allo SCT is a valuable clinical option for patients with 1st relapse after HDM and auto SCT.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal