

Abstract
Abstract 3768
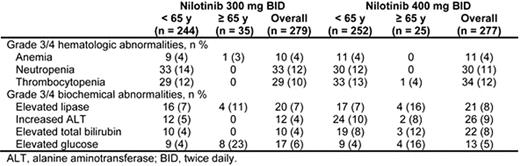
Data from the phase 3, randomized multicenter ENESTnd trial have demonstrated the superiority of nilotinib over imatinib after 24 months (mo) of follow-up, with significantly higher rates of complete cytogenetic response (CCyR) and major molecular response (MMR), and significantly lower rates of progression to accelerated phase/blast crisis (AP/BC). The current subanalysis evaluated the efficacy and safety of nilotinib 300 mg twice daily (Nil300) and nilotinib 400 mg twice daily (Nil400) in older (≥ 65 years [yrs] at study entry) patients (pts) with newly diagnosed chronic myeloid leukemia (CML) in chronic phase (CP) with a minimum follow-up of 24 mo. Methods: In ENESTnd, 846 pts stratified by Sokal risk score were randomized 1:1:1 to Nil300 (n = 282), Nil400 (n = 281), or imatinib 400 mg once daily (n = 283). Pts with impaired cardiac function or ECOG performance status > 2 were excluded. Rates of CCyR and MMR by 24 mo, progression to AP/BC on treatment, and safety were evaluated according to age group (< 65 vs ≥ 65 yrs) in the 2 nilotinib arms. Safety data are reported for any pt who received ≥ 1 dose of nilotinib (n = 279, Nil300; n = 277, Nil400). Results: 36 pts (13%) and 28 pts (10%) were ≥ 65 yrs old in the Nil300 and Nil400 arms, respectively. Of the pts aged ≥ 65 yrs, 51/64 (80%) had an ECOG performance status of 0 at baseline and 60/64 (94%) had intermediate or high Sokal risk scores. Of the older pts, 8 (22%) on Nil300 and 6 (21%) on Nil400 had type 2 diabetes at baseline. CCyR rates by 24 mo were 83% and 68% among older pts treated with Nil300 and Nil400, respectively, and 87% for pts aged < 65 yrs in each nilotinib arm. By 24 mo, MMR was achieved by 72% and 61% of older pts on Nil300 and Nil400, respectively; in pts aged < 65 yrs, the respective rates were 71% and 67%. All 5 pts who progressed to AP/BC on treatment (2 on Nil300 and 3 on Nil400) were aged < 65 yrs. The frequency of grade 3/4 hematologic adverse events (AEs) was low in older pts; no pts had grade 3/4 neutropenia and only 1 older pt reported grade 3/4 thrombocytopenia in each nilotinib arm (Table). Transient, asymptomatic lipase elevations were reported in 11% and 16% of older pts treated with Nil300 and Nil400, and 7% of younger pts in each arm. Hyperglycemia occurred in 23% and 16% of older pts on Nil300 and Nil400, respectively, and 4% of younger pts in each arm; regardless of age, no pt discontinued study due to hyperglycemia. Among the 12 older pts with grade 3/4 hyperglycemia (8 on Nil300; 4 on Nil400), 9 pts had type 2 diabetes at baseline. There were no QTcF increases of > 60 msec from baseline in older pts and 3 in nilotinib-treated pts < 65 yrs old (1 on Nil300; 2 on Nil400). QTcF prolongation of > 500 msec did not occur in any pt treated with nilotinib on study. Periodic echocardiograms were done, and there were no decreases of > 15% in left ventricular ejection fraction from baseline in any pt treated with nilotinib on study. There were 4 cases of ischemic heart disease reported in older pts (1/35 [3%] on Nil300; 3/25 [12%] on Nil400) and 7 cases in pts < 65 yrs of age (4/244 [2%] on Nil300; 3/252 [1%] on Nil400). No sudden deaths occurred on study. Discontinuation occurred in approximately 25% of older and younger pts with Nil300, of which, 6% and 9%, respectively, were due to AEs/lab abnormalities. Discontinuation from study with Nil400 was 46% in older pts and 19% in younger pts; of which, 36% and 10% were due to AEs/lab abnormalities. Conclusions: Older pts treated with nilotinib demonstrated high rates of cytogenetic and molecular responses and low rates of progression. Nilotinib was generally well tolerated by older pts. In older pts, Nil300 had numerically higher rates of CCyR and MMR and was generally better tolerated (as evidenced by fewer AEs and discontinuations) vs Nil400. These data support the use of Nil300 in older pts with newly diagnosed CML-CP.
Larson:Novartis Pharmaceuticals: Consultancy, Honoraria, Research Funding. Bunworasate:Novartis Pharmaceutical: Research Funding. Turkina:Novartis: Consultancy, Honoraria; BMS: Honoraria. Goldberg:Bristol Myers Squibb: Honoraria, Research Funding, Speakers Bureau; Novartis Pharmaceutical: Honoraria, Research Funding, Speakers Bureau; Ariad: Research Funding. Dorlhiac-Llacer:Bristol Myers Squibb: Research Funding; Novartis: Research Funding. Kantarjian:Novartis: Consultancy; Novartis: Research Funding; Pfizer: Research Funding; BMS: Research Funding. Saglio:Bristol-Myers Squibb: Consultancy, Speakers Bureau; Novartis Pharmaceutical: Consultancy, Speakers Bureau; Pfizer: Consultancy. Hochhaus:Ariad: Consultancy, Honoraria, Research Funding; Bristol Myers Squibb: Consultancy, Honoraria, Research Funding; Novartis Pharmaceutical: Consultancy, Honoraria, Research Funding; Merck: Consultancy, Honoraria, Research Funding. Hoenekopp:Novartis Pharmaceutical: Employment, Equity Ownership. Blakesley:Novartis Pharmaceutical: Employment. Yu:Novartis: Employment, Equity Ownership. Gallagher:Novartis: Employment, Equity Ownership. Clark:Bristol Myers Squibb: Honoraria, Research Funding; Novartis Pharmaceutical: Honoraria, Research Funding, Speakers Bureau. Hughes:Bristol Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Ariad: Honoraria, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal